New preprint: "PopART-IBM, a highly efficient stochastic individual-based simulation model of generalised HIV epidemics developed in the context of the HPTN 071 (PopART) trial" with Mike Pickles, @dr_anne_cori @p_robot and friends. 1/n medrxiv.org/content/10.110…
A few years we found we needed an agent based model to simulate interventions against the HIV pandemic in southern Africa, and ended up developing a new one. We found that with heterogeneities and detailed interventions, ABMs were more parsimonious than compartmental models. 2/n
So we set out to develop a model that was, to paraphrase, "as simple as necessary, but no simpler". We wanted it to be computationally efficient so as to be able to do parameter sweeps and inference. Here it is 3/n github.com/BDI-pathogens/…
It simulates what we think we needed. A lot of parameters and computations are linked to the dynamic sexual network. 4/n 

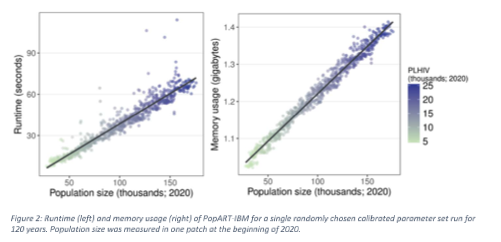
It's pretty nifty on a laptop. 5/n
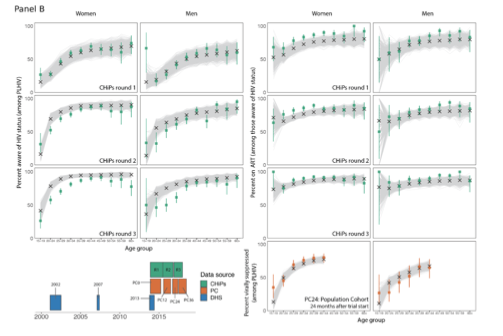
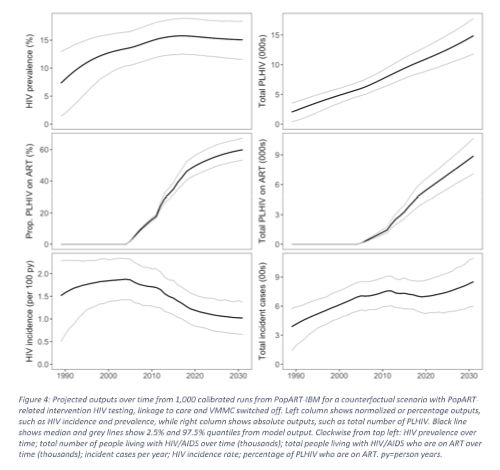
You can do Bayesian fitting to a whole lot of summary statistics 6/n.
Epidemic curves describe the epidemic in the communities where we working in Zambia and South Africa. The numbers are always quite shocking. 7/n
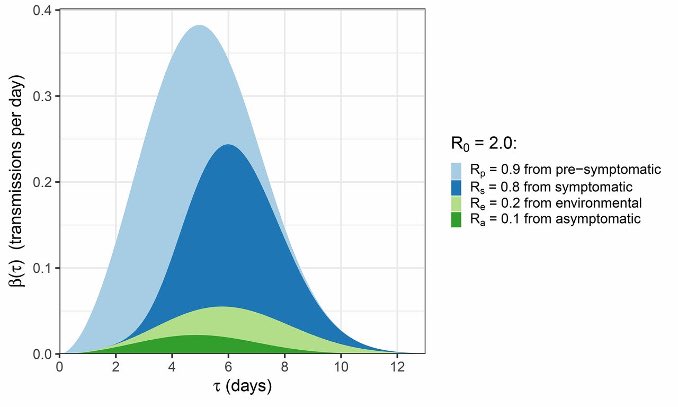
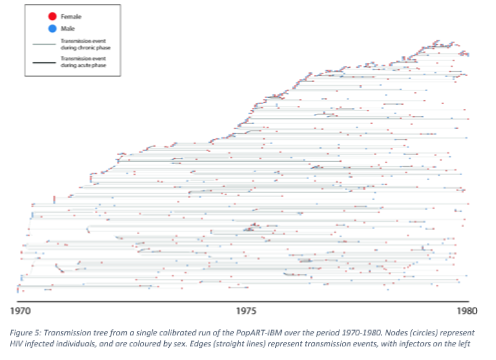
The model simulates individual transmission events, and the best fit epidemics have an interesting mix of transmission types, with two visible tempi of transmission. Clusters of rapid transmission, interspersed with long periods before the next cluster. 8/n
The model has limitations. Only heterosexual transmission is modelled. There are no key populations. 9/n
Recently, Rob Hinch has been re-coding to make it easier to make changes. Some of the coding concepts have made it into our COVID-19 simulator. 10/n github.com/BDI-pathogens/…
The work was done together with many wonderful collaborators from the HPTN 071 PopART trial 11/n nejm.org/doi/full/10.10…
Coming soon: to test the predictive ability of the model, we posted predictions from the model before the trial was unblinded. We will publish this alongside some learnings from re-fitting the model to the trial outcome. 12/end
Postscript 1: we welcome collaboration on using & extending this model. Our recent experience with OpenABM-Covid-19 shows that with generic network simulation, custom transmission and interventions, and a strong unit testing framework, this code is ready for collaboration. 13/12
• • •
Missing some Tweet in this thread? You can try to
force a refresh