
1/x Pt w/dialysis-dependent AKI arrives from LTAC w/severe acute hypernatremia (166). High GI output is deemed possibly causative. H/o pancreatic/duodenal fístula and PEG. Loss of hypotonic fluids and limited access to water seemed plausible. Let’s look at the rest of the BMP... 
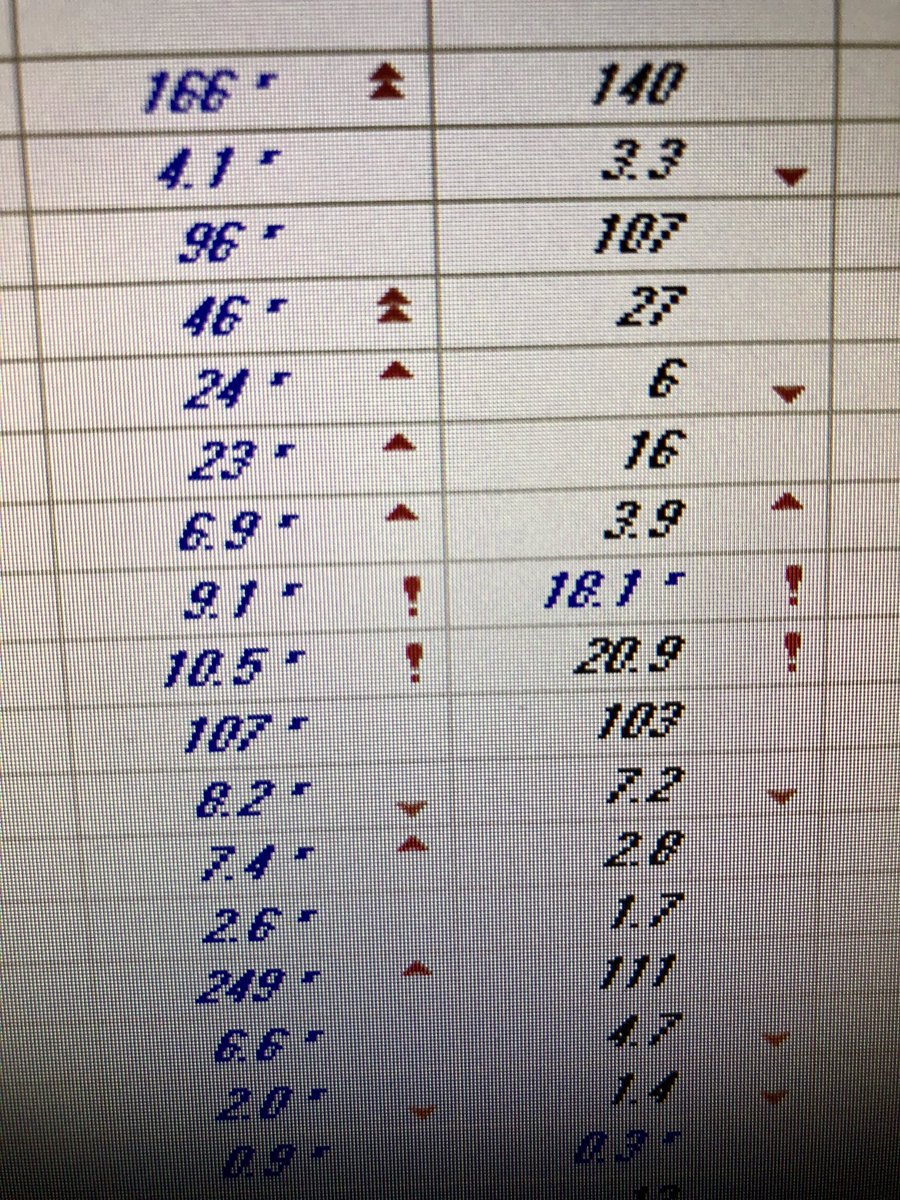
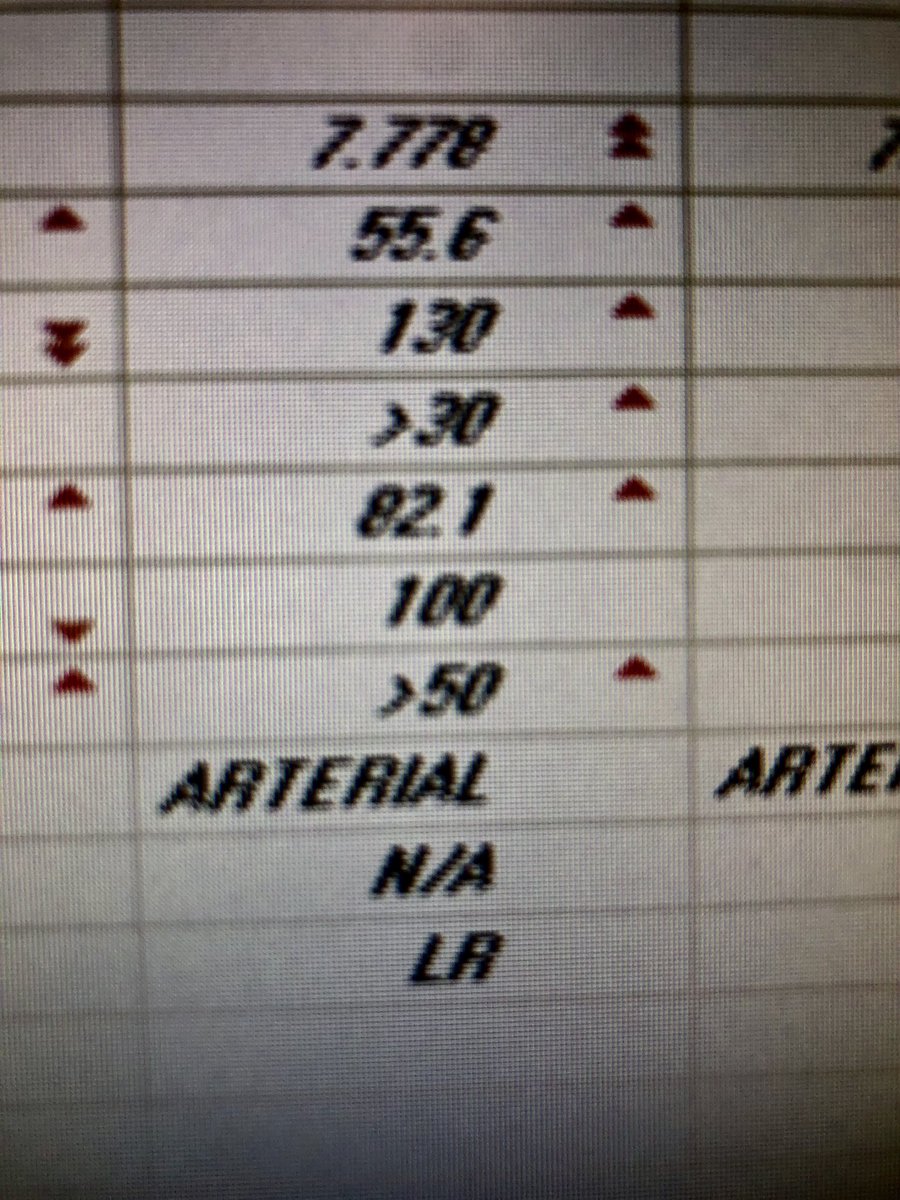
2/x the high CO2 (46) suggests met alkalosis. Now, that’s unexpected in a pt with GI losses from supposedly a duodenal fistula. Could he just be a CO2 retainer? Well the ABG confirmed primary met alkalosis. Calculated HCO3 82! That’s a personal record. UOP <400cc/d; no diuretics
3/x a logical hypothesis was high output from PEG to suction. Not the case. Pt being fed 4 comfort ~ 1 L/day. But output from enteric fistula was 3-4 L/day. Upon reading Surg report, there was a note about a jejunal “hole”. Does it matter if fistula is duodenal, ileal or jejunal?
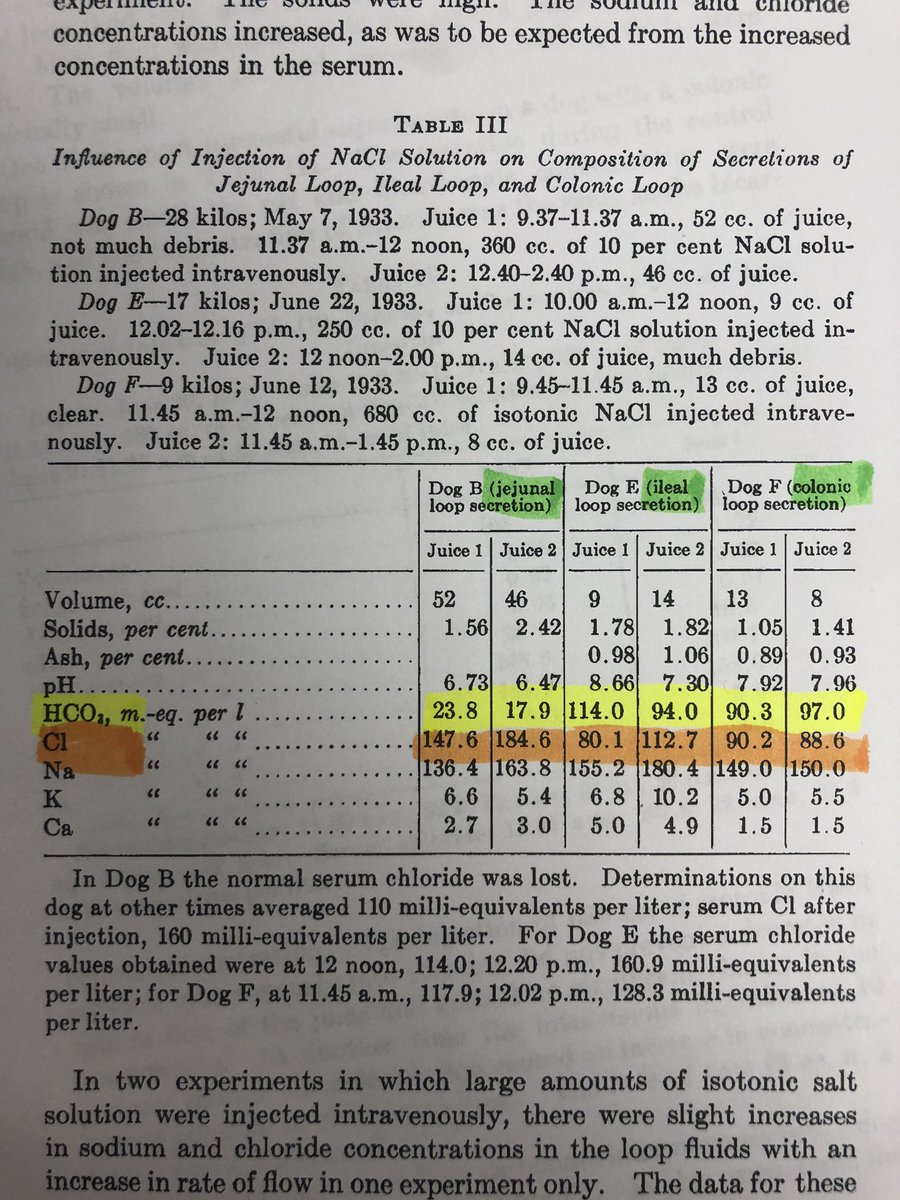
4/x love digging those old papers. Here we can see that, as expected, ileal and colonic fluid is rich in HCO3 and relatively low in Cl (compared to plasma).

5/x here it gets interesting. Look at the low HCO3 and high Cl concentration in the jejunal fluid of these dogs! So that would suggest that jejunal fluid loss could lead to hypochloremia and met alkalosis. Contacted surgeon. They insisted that fistula was duodenal 🤔
6/x is it possible that somehow the duodenal epithelia has dedifferentiated and is now spilling Cl instead of HCO3? Indeed, acquired chloridorrhea has been reported after bowel surgery and in IBD pubmed.ncbi.nlm.nih.gov/25874098/ pubmed.ncbi.nlm.nih.gov/14655202/ essentially the Cl-HCO3 flips
7/x at that point, a way 2 find out: measure lytes in GI fluid: Na <100 (it explains hyperNa), CO2 <5!, Cl 116! So there you go. Massive chloride loss led to this whooping degree of metabolic alkalosis. Background of AKI-RRT negated a way to exchange Cl 4 HCO3 by IC-B cells w/NS
8/8 pt was managed with D5W IV and then HD: bicarb bath 25, no UF. Bicarb kept 28-32 after 2 sessions. GI output eventually slowed down. Mental status was never down. Tolerance to alkalemia always amazes me.
@alhosaini_nour 👆take q look
This case was not about dialysis, but in case anybody wonders, pH improved from 7.78 to 7.46 after a 6-hr SLED Run.

