#GUPath twitter brain trust. Posting for a colleague.
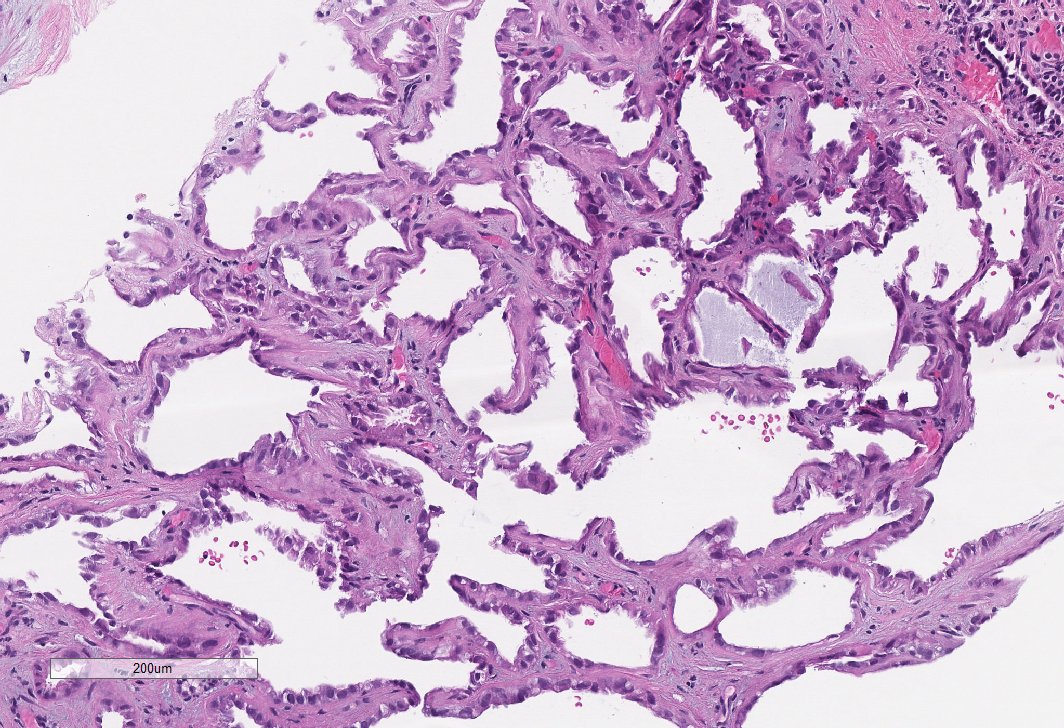
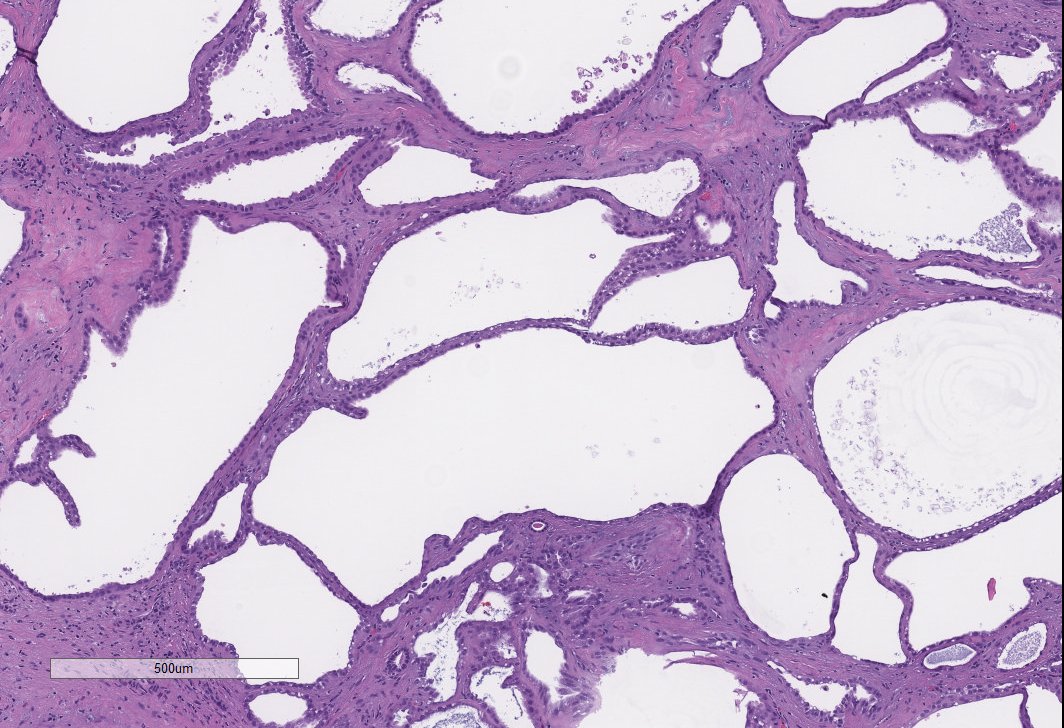
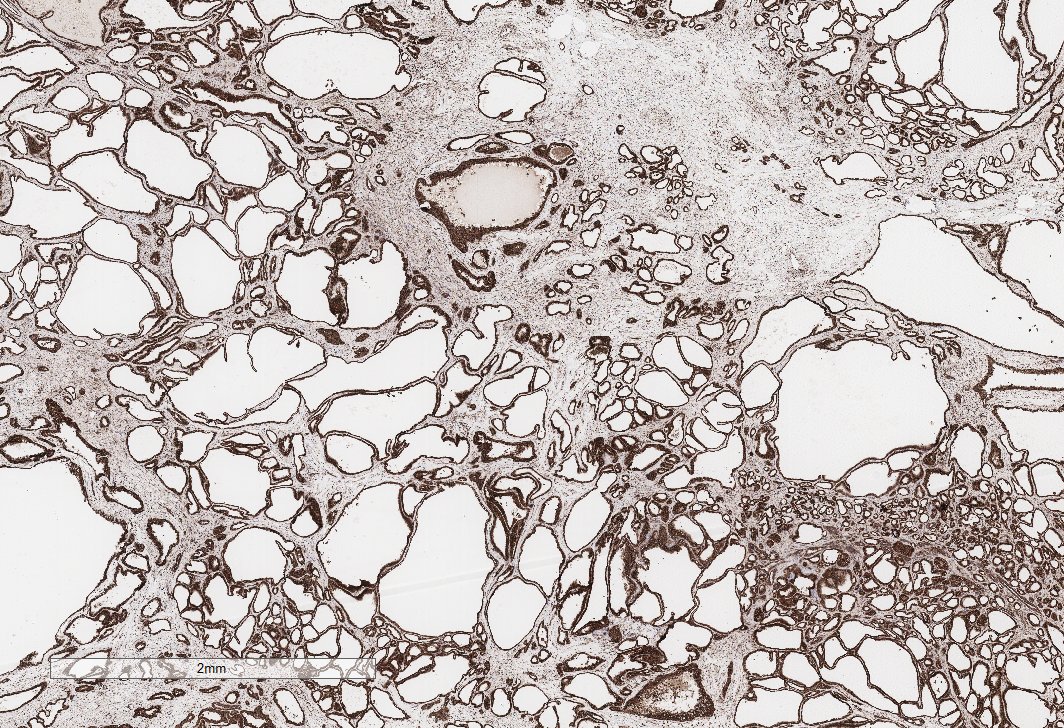
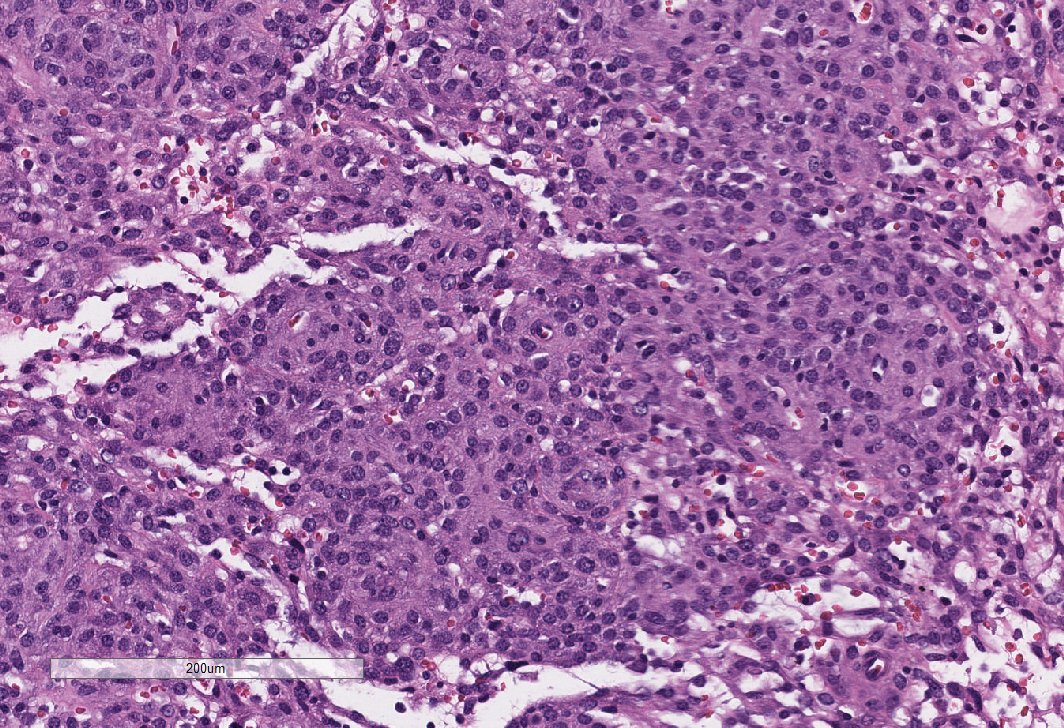
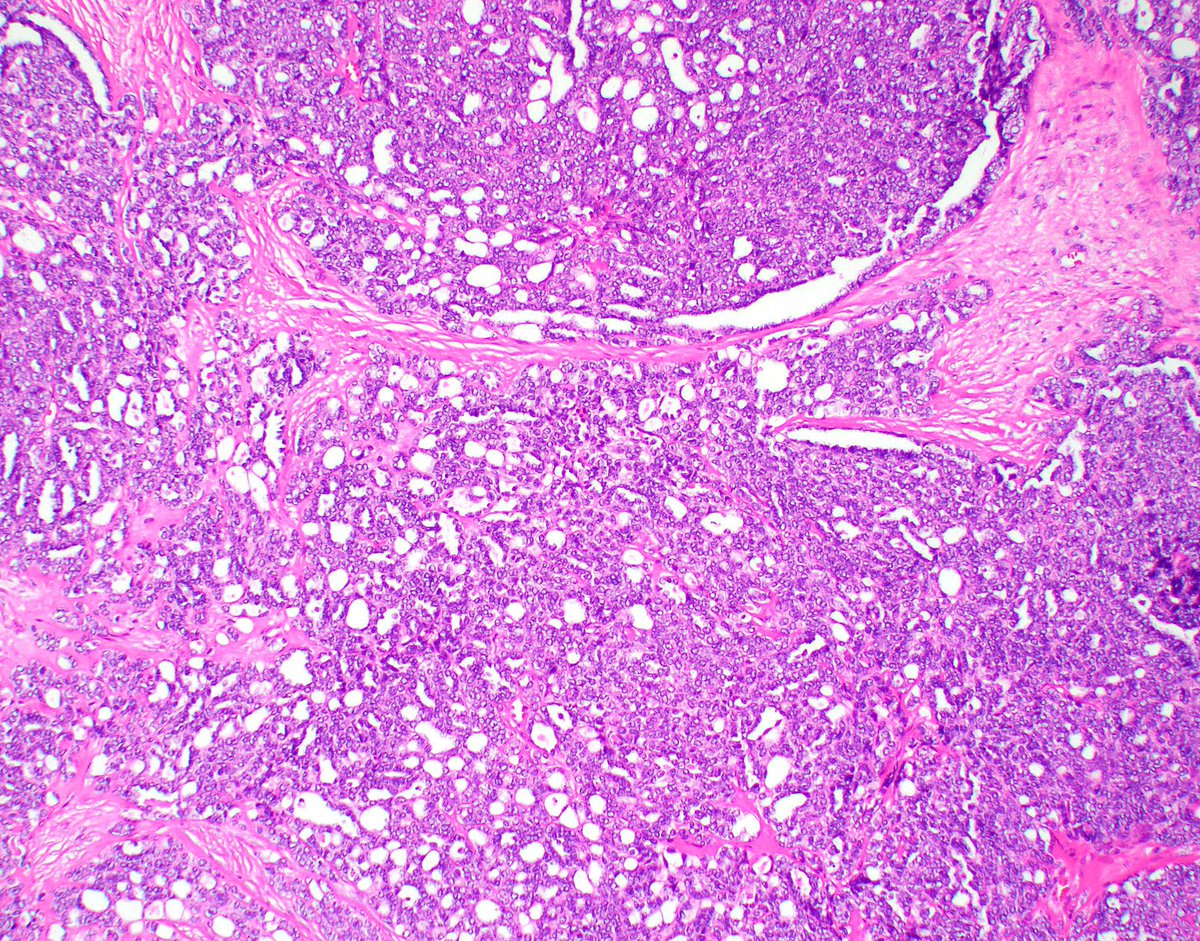
37yo man with a renal mass.
Pos for PAX8, keratin. Neg for NE markers, GATA, WT1 and everything else.
We are stumped. Thoughts? Anyone seen something like this before? We thought of adult Wilms’s but IHC doesn’t support.
37yo man with a renal mass.
Pos for PAX8, keratin. Neg for NE markers, GATA, WT1 and everything else.
We are stumped. Thoughts? Anyone seen something like this before? We thought of adult Wilms’s but IHC doesn’t support.



@Williamson_SR @Kiril_T_Can @johncheville @rovingatuscap @MichelleDunno17 @FionaMacPath @daniel_berney #GUPath
Tumor is primary to the kidney. He’s older and PAX8 +++ so we didn’t think this was teratoma. I did consider it briefly.
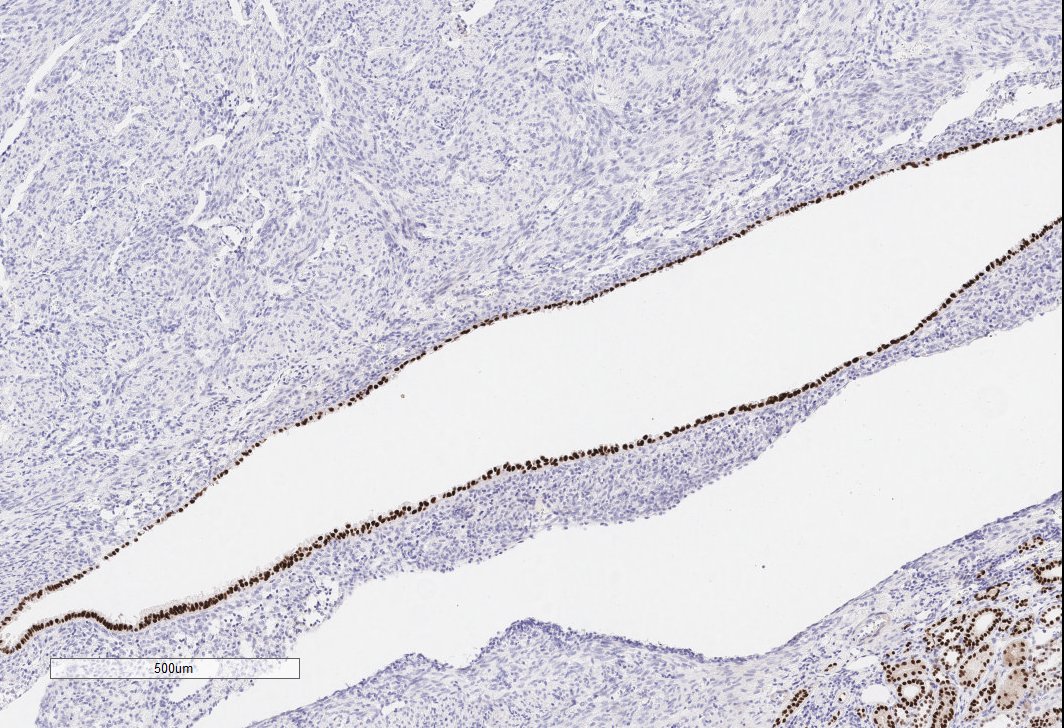
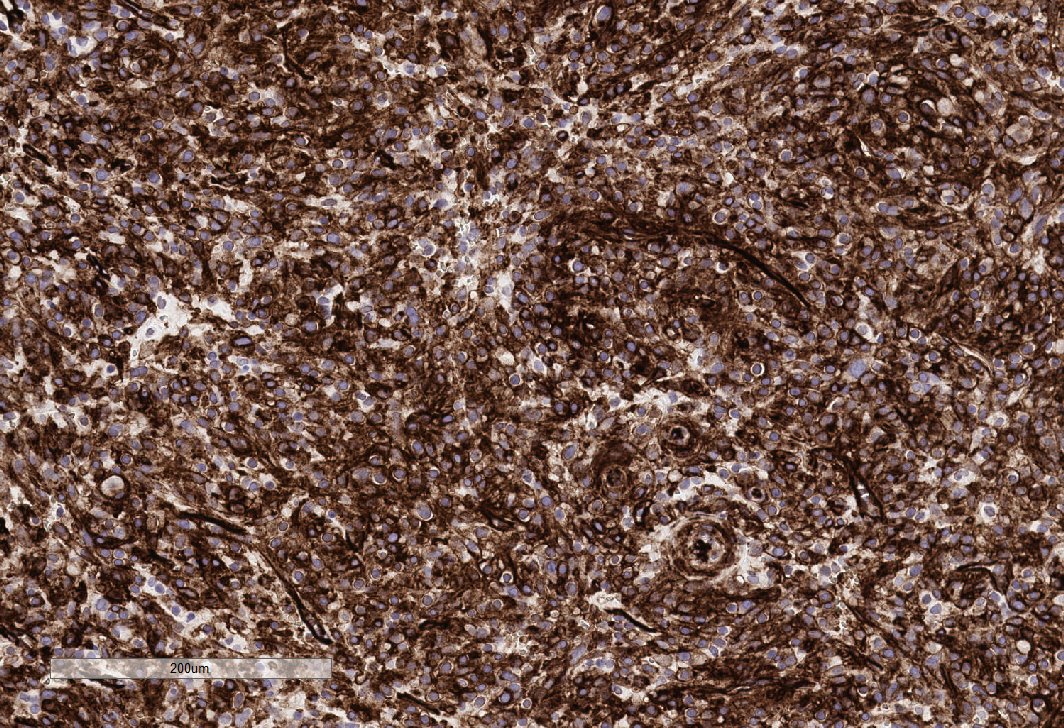
Positive:
PAX-8 (strong), CK cocktail, CK 7, CK 8/18, CK 19, vimentin (focal), EMA, CD10 (membranous), E-cadherin. INI-1 intact. P53 + in 10% of tumor. P504S, CD56 and synaptophysin weak and focal.
PAX-8 (strong), CK cocktail, CK 7, CK 8/18, CK 19, vimentin (focal), EMA, CD10 (membranous), E-cadherin. INI-1 intact. P53 + in 10% of tumor. P504S, CD56 and synaptophysin weak and focal.
Negative:
RCC, OCT 3/4, p63, cytokeratin 34betaE1 (rare), WT1, chromogranin, CD57, TTF1, Thyroglobulin, NKX3.1, CDX2, TLE1, Beta-Catenin, SALL4, cytokeratin 20 and TFE-3.
RCC, OCT 3/4, p63, cytokeratin 34betaE1 (rare), WT1, chromogranin, CD57, TTF1, Thyroglobulin, NKX3.1, CDX2, TLE1, Beta-Catenin, SALL4, cytokeratin 20 and TFE-3.
• • •
Missing some Tweet in this thread? You can try to
force a refresh