Should GI symptoms (abdo pain, diarrhoea, vomiting) be included in the case definition for #COVID19 in children?
Lots of questions prompted by a new paper from my colleague Tom Waterfield et al.
If only there were simple answers....
medrxiv.org/content/10.110…
1/9
Lots of questions prompted by a new paper from my colleague Tom Waterfield et al.
If only there were simple answers....
medrxiv.org/content/10.110…
1/9
The question has come from this table, which found of children who tested positive vs negative for SARS-CoV-2 IgG, GI symptoms were associated with testing positive
You'll note the exact same is true of headache, which was just as common
2/9
You'll note the exact same is true of headache, which was just as common
2/9
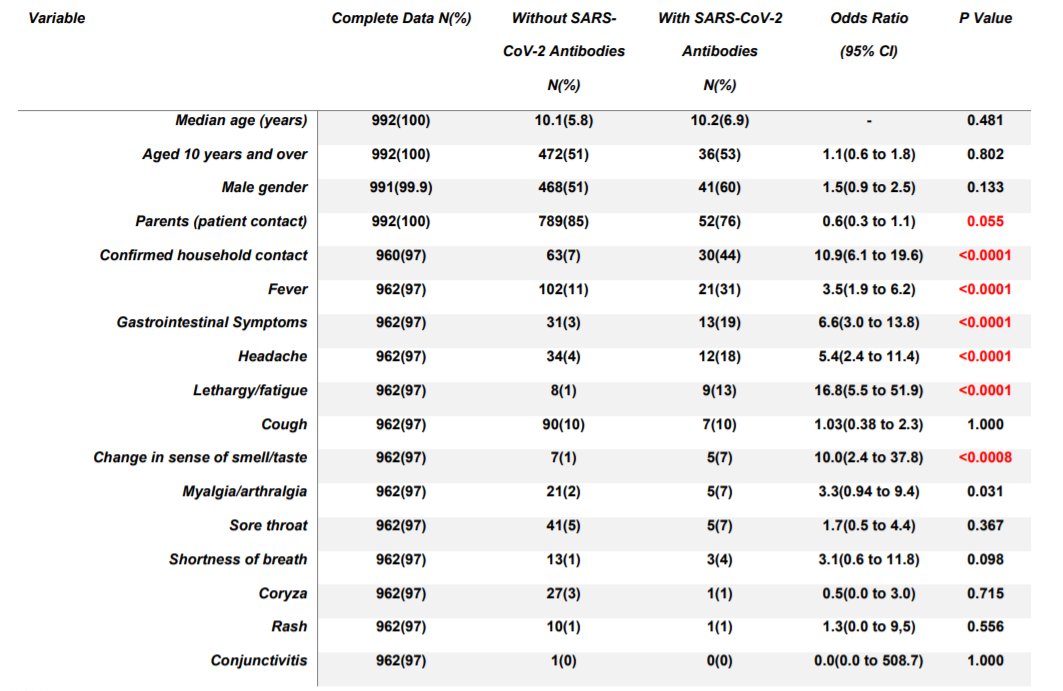
We've known for a long time COVID-19 can present with abdominal symptoms in both children and adults, although it may be slightly more common in children
Here only 20% of children with antibodies had GI symptoms; this is higher than cough (10%!) but lower than fever (31%)
3/9
Here only 20% of children with antibodies had GI symptoms; this is higher than cough (10%!) but lower than fever (31%)
3/9
So should we use this in our case definition?
Well it's not an easy question
This study was in spring when GI bugs are at their lowest, so competing diagnoses were less prevalent. In winter, this may tip it out of favour as discriminating for COVID.
4/9
Well it's not an easy question
This study was in spring when GI bugs are at their lowest, so competing diagnoses were less prevalent. In winter, this may tip it out of favour as discriminating for COVID.
4/9
We also need to know about symptom cross over; if 100% of children with GI symptoms also have fever, adding GI symptoms won't increase pick up but will add extra non-COVID patients to our basket (just more negative tests clogging the system)
5/9
5/9
We are already nearly at testing capacity, so adding 1000's of children per week who vomit a couple of times over winter could completely collapse the system
Would they even test positive via NP/OP sampling?
Stool can test +ve for weeks, would they still be infectious?
6/9
Would they even test positive via NP/OP sampling?
Stool can test +ve for weeks, would they still be infectious?
6/9
We quickly need a directive on the goal of targeted testing for children
50% are asymptomatic. Can we add in hundreds of thousands of tests for GI symptoms to pick up a handful of cases?
7/9
50% are asymptomatic. Can we add in hundreds of thousands of tests for GI symptoms to pick up a handful of cases?
7/9
Are we testing to;
- Get kids out of quarantine back in to school
- Pick up the most symptomatic or ?contagious cases
- Promote contact tracing
- ?other
We can't find them all; half have no symptoms, and the rest are very vague and cross over every other virus in children
8/9
- Get kids out of quarantine back in to school
- Pick up the most symptomatic or ?contagious cases
- Promote contact tracing
- ?other
We can't find them all; half have no symptoms, and the rest are very vague and cross over every other virus in children
8/9
Also, do we need a different criteria in adolescents to younger children (<10y)?
Difficult questions which need careful thinking and planning - including estimate for burdens on capacity
Much to think about here. No quick solutions.
9/9
Difficult questions which need careful thinking and planning - including estimate for burdens on capacity
Much to think about here. No quick solutions.
9/9
• • •
Missing some Tweet in this thread? You can try to
force a refresh