1/14
Why do we feel cold (i.e., experience "chills") when we have a fever? Shouldn't we feel hot?
And what are rigors?
Answers to these questions will help us better understand when we should obtain blood cultures.
When do you think is the best time to draw them?
Why do we feel cold (i.e., experience "chills") when we have a fever? Shouldn't we feel hot?
And what are rigors?
Answers to these questions will help us better understand when we should obtain blood cultures.
When do you think is the best time to draw them?
2/
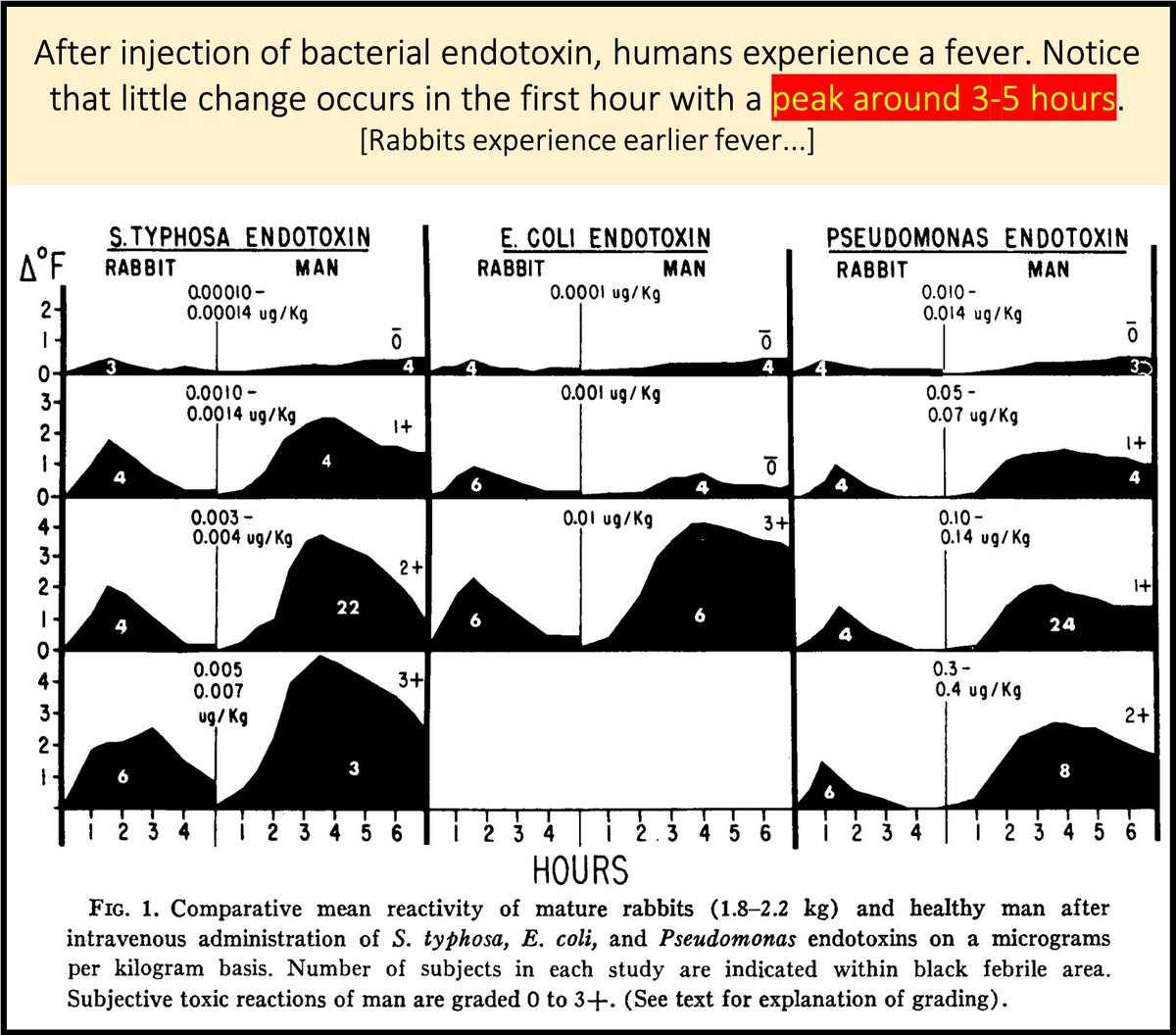
Bacteremia exposes us to exogenous pyrogens. For example, the cell wall of gram-negative rods contains lipopolysaccharide (LPS; endotoxin).
When injected into humans LPS induces fever. But, there is a 3-5 hour delay between exposure and peak fever.
pubmed.ncbi.nlm.nih.gov/4897836/
Bacteremia exposes us to exogenous pyrogens. For example, the cell wall of gram-negative rods contains lipopolysaccharide (LPS; endotoxin).
When injected into humans LPS induces fever. But, there is a 3-5 hour delay between exposure and peak fever.
pubmed.ncbi.nlm.nih.gov/4897836/
3/
The delay between clinical bacteremia and fever was demonstrated in 1932 by Weiss and Ottenberg.
Their conclusion: Obtain blood cultures BEFORE fever. If only it were easy to predict future fevers!
[Maybe we can as you'll see in tweet 10 below.]
academic.oup.com/jid/article-ab…
The delay between clinical bacteremia and fever was demonstrated in 1932 by Weiss and Ottenberg.
Their conclusion: Obtain blood cultures BEFORE fever. If only it were easy to predict future fevers!
[Maybe we can as you'll see in tweet 10 below.]
academic.oup.com/jid/article-ab…
4/
Why is there a delay between bacteremia and fever?
There's a lot to be done!
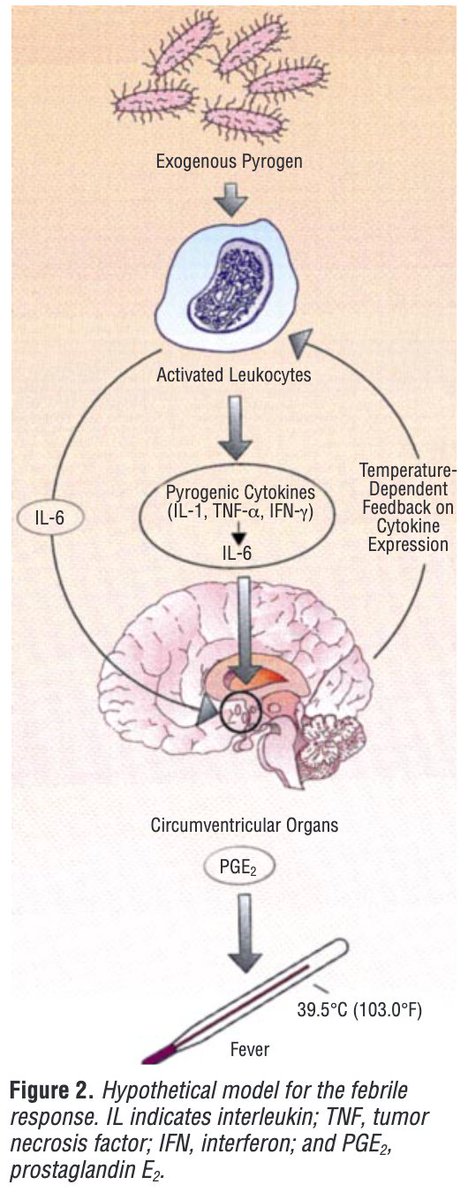
◾️LPS induces endogenous pyrogens (e.g., IL-6) which...
◾️Increase the hypothalamic set-point, resulting in...
◾️Thermogenesis, vasoconstriction, etc., and...
◾️Fever
pubmed.ncbi.nlm.nih.gov/9759682/
Why is there a delay between bacteremia and fever?
There's a lot to be done!
◾️LPS induces endogenous pyrogens (e.g., IL-6) which...
◾️Increase the hypothalamic set-point, resulting in...
◾️Thermogenesis, vasoconstriction, etc., and...
◾️Fever
pubmed.ncbi.nlm.nih.gov/9759682/
5/
During this period between bacteremia and fever we may feel cold (i.e., we experience chills).
Why? There are at least two possible explanations.
1⃣Peripheral vasoconstriction → fall in skin temperature → "I'm cold!"
2⃣Direct central signal → "I'm cold!"
Which is it?
During this period between bacteremia and fever we may feel cold (i.e., we experience chills).
Why? There are at least two possible explanations.
1⃣Peripheral vasoconstriction → fall in skin temperature → "I'm cold!"
2⃣Direct central signal → "I'm cold!"
Which is it?
6/
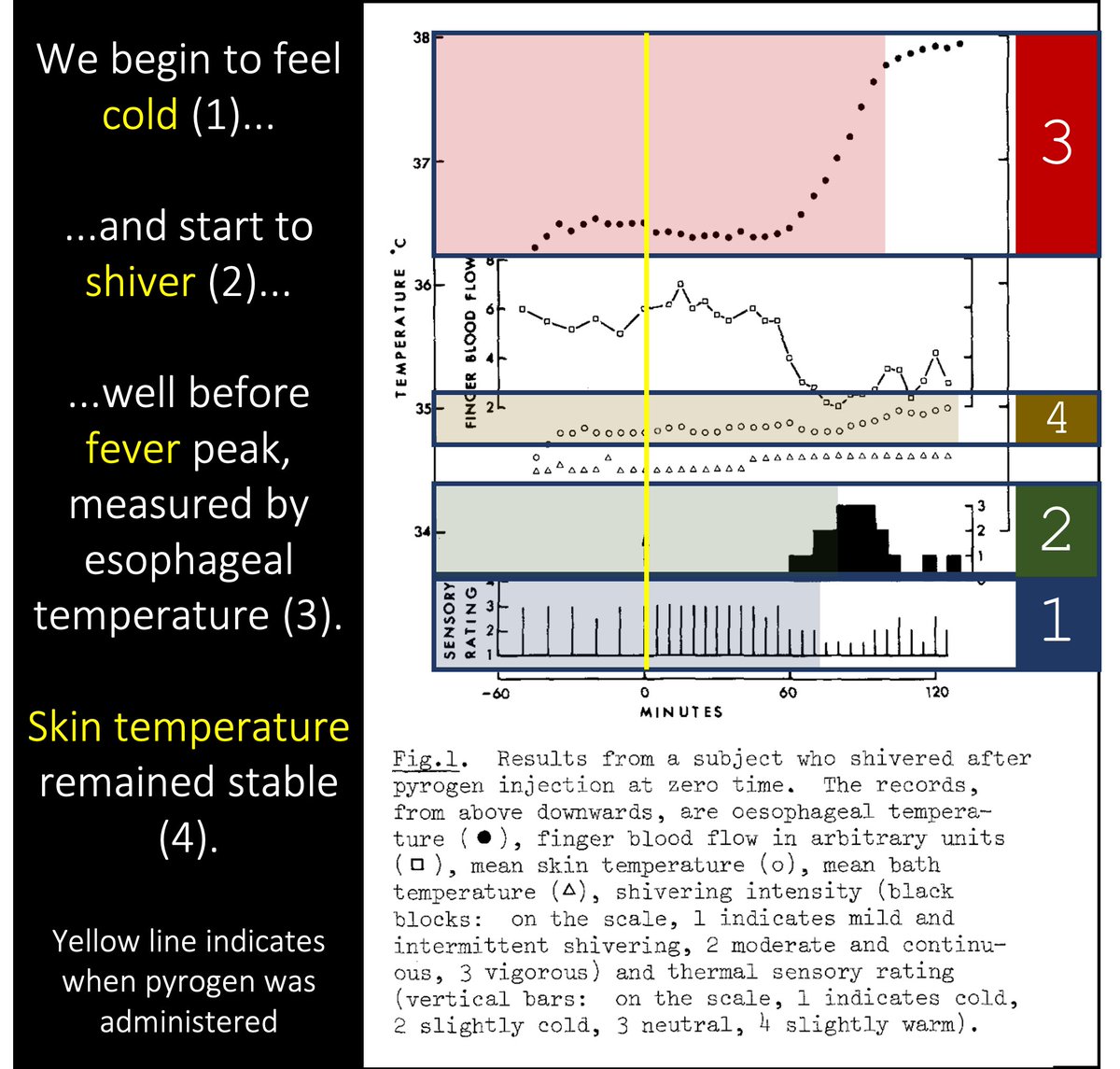
In one study, subjects were placed in water at a stable temperature and injected with a pyrogen.
Before fever, they felt cold. This was despite a stable skin temperature.
🔑chills must therefore arise from some central action of pyrogens
pubmed.ncbi.nlm.nih.gov/7189863/
In one study, subjects were placed in water at a stable temperature and injected with a pyrogen.
Before fever, they felt cold. This was despite a stable skin temperature.
🔑chills must therefore arise from some central action of pyrogens
pubmed.ncbi.nlm.nih.gov/7189863/
7/
Why would an "I'm cold!" signal be sent?
This signal drives behavioral changes that aid with heat retention as our body aims to raise core temperature.
"I'm cold!" propels us to put on a blanket, seek shelter, etc.
🔑We ARE cold compared with what our body wants us to be!
Why would an "I'm cold!" signal be sent?
This signal drives behavioral changes that aid with heat retention as our body aims to raise core temperature.
"I'm cold!" propels us to put on a blanket, seek shelter, etc.
🔑We ARE cold compared with what our body wants us to be!
8/
If we require a rapid increase in temperature we might also experience violent shivering.
aka shaking chills
aka RIGORS
The muscle contractions of rigors result in rapid heat production (thermogenesis) aiding fever onset.
pubmed.ncbi.nlm.nih.gov/14405791/
If we require a rapid increase in temperature we might also experience violent shivering.
aka shaking chills
aka RIGORS
The muscle contractions of rigors result in rapid heat production (thermogenesis) aiding fever onset.
pubmed.ncbi.nlm.nih.gov/14405791/
9/
We don't always require the rapid-onset fever that rigors produce. But bacteremia is a scenario where it might make sense.
So, is there an association between rigors and bacteremia?
Yes!
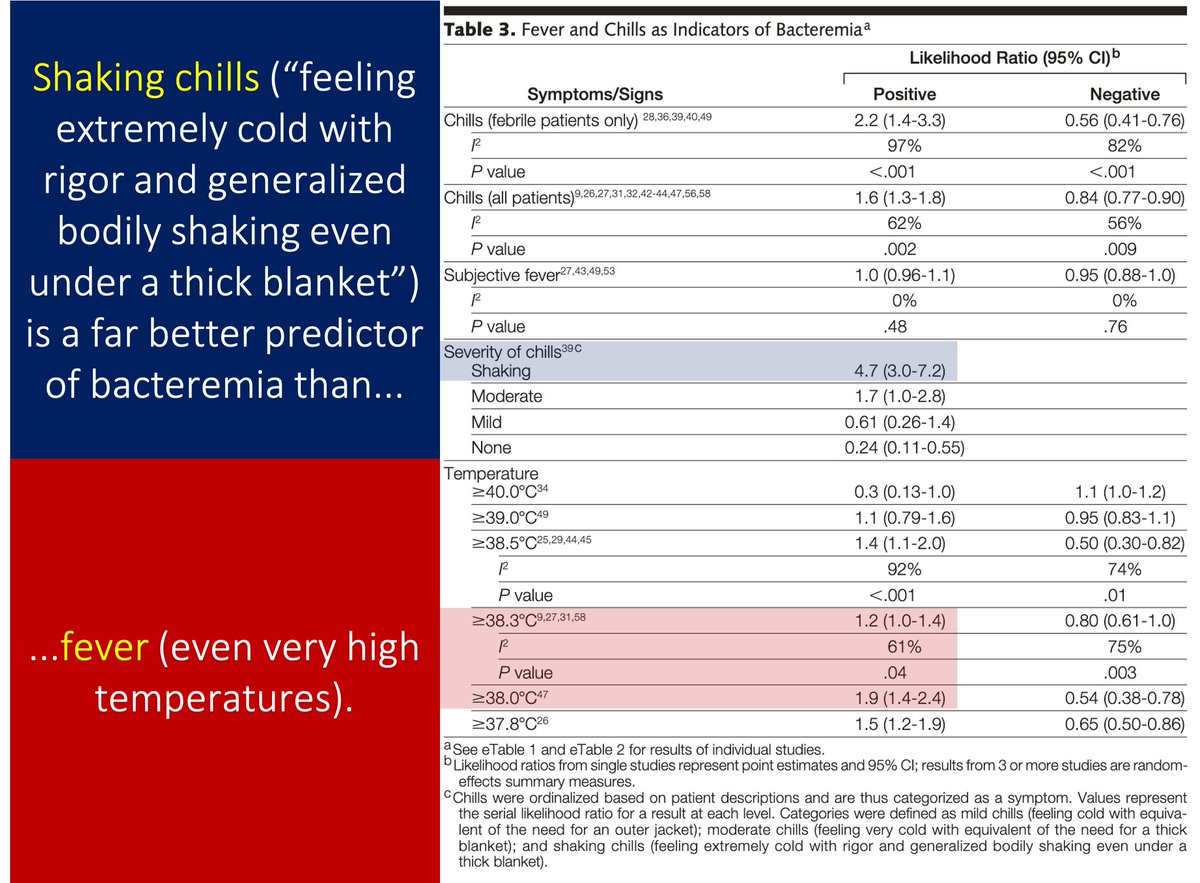
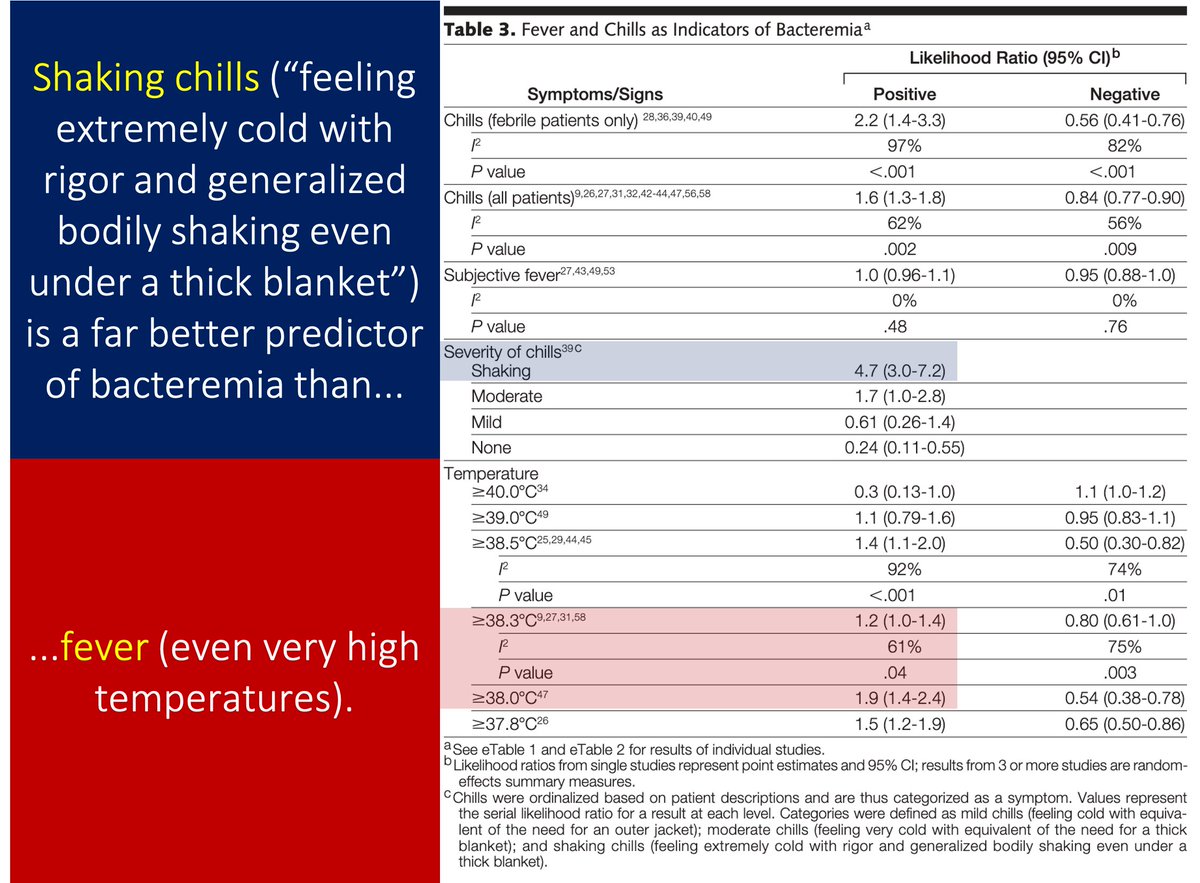
In fact, rigors predictor bacteremia better than fever.
pubmed.ncbi.nlm.nih.gov/22851117/
We don't always require the rapid-onset fever that rigors produce. But bacteremia is a scenario where it might make sense.
So, is there an association between rigors and bacteremia?
Yes!
In fact, rigors predictor bacteremia better than fever.
pubmed.ncbi.nlm.nih.gov/22851117/
10/
Should we say "culture if shakes" instead of "culture if spikes"?
Maybe. Remember the order of events:
1⃣Bacteremia
2⃣Increased temperature set-point
3⃣"I'm cold" and4⃣Rigors
5⃣Fever
Chills and rigors should appear before a fever. And closer to the bacteremia.
Should we say "culture if shakes" instead of "culture if spikes"?
Maybe. Remember the order of events:
1⃣Bacteremia
2⃣Increased temperature set-point
3⃣"I'm cold" and4⃣Rigors
5⃣Fever
Chills and rigors should appear before a fever. And closer to the bacteremia.
11/
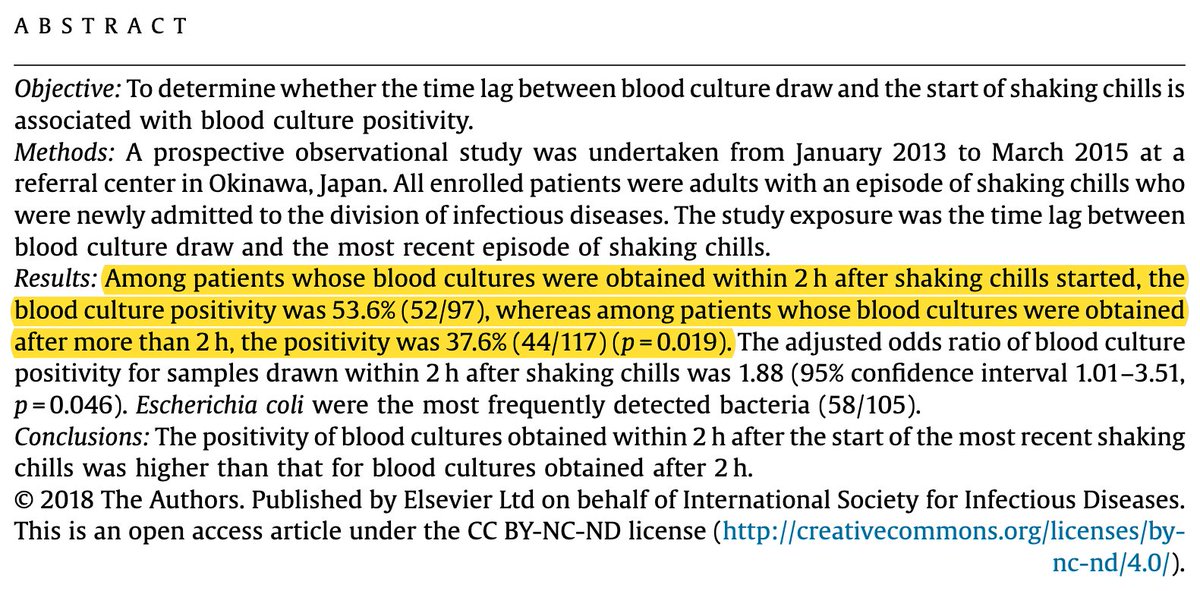
While rigors occur closer to bacteremia than fever (and therefore better predict positive cultures), there is still a delay. They're not perfect.
But, if you obtain blood cultures within 2 hours of rigors there is increased likelihood of positivity.
pubmed.ncbi.nlm.nih.gov/30059771/
While rigors occur closer to bacteremia than fever (and therefore better predict positive cultures), there is still a delay. They're not perfect.
But, if you obtain blood cultures within 2 hours of rigors there is increased likelihood of positivity.
pubmed.ncbi.nlm.nih.gov/30059771/
12/
Before concluding, let me re-ask a version of the original question.
If you could obtain blood cultures at any of the following periods, which would you choose?
Before concluding, let me re-ask a version of the original question.
If you could obtain blood cultures at any of the following periods, which would you choose?
13/ - SUMMARY - Part 1
🔳The order of events: bacteremia and exogenous pyrogen exposure → increase temperature set-point → chills/rigors → fever
🔳We may feel cold chills as a cue to drive behavioral change (e.g., put on a sweater)
🔳Rigors promote rapid heat production
🔳The order of events: bacteremia and exogenous pyrogen exposure → increase temperature set-point → chills/rigors → fever
🔳We may feel cold chills as a cue to drive behavioral change (e.g., put on a sweater)
🔳Rigors promote rapid heat production
14/14 - SUMMARY - Part 2
🔳By the time fever occurs, bacteremia may have already cleared
🔳Because rigors occur before fever (i.e., temporally closer to bacteremia), they are better predictors of positive blood cultures
🔳Neither is perfect
🔳By the time fever occurs, bacteremia may have already cleared
🔳Because rigors occur before fever (i.e., temporally closer to bacteremia), they are better predictors of positive blood cultures
🔳Neither is perfect
• • •
Missing some Tweet in this thread? You can try to
force a refresh