(1/)I've had several people ask me about details on how to use bedside ultrasound to confirm ET tube placement, detect esophageal and mainstem intubations, and adjust positioning.
So here is a step by step guide!
Ref: journals.lww.com/ccejournal/Ful…
So here is a step by step guide!
Ref: journals.lww.com/ccejournal/Ful…
(2/)**Overview** this protocol utilizes sequential tracheal and bilateral thoracic lung ultrasound.
1. Tracheal ultrasound to r/o esophageal intubations
2. Right Lung US
3. Left Lung US
4. Adjustment to achieve bilateral lung sliding
1. Tracheal ultrasound to r/o esophageal intubations
2. Right Lung US
3. Left Lung US
4. Adjustment to achieve bilateral lung sliding

(3/)**Tracheal Ultrasound**
This is simple. Place your transducer transversely at the level of the suprasternal notch. Below is an example of the appearance of the trachea with a hyperechoic anterior wall and acoustic shadowing.
This is simple. Place your transducer transversely at the level of the suprasternal notch. Below is an example of the appearance of the trachea with a hyperechoic anterior wall and acoustic shadowing.

(4/) Know your paratracheal structures well! Also familiarize yourself with the appearance using the linear transducer or phased array/abdominal probe. Pay special attention to the left paratracheal region where an often collapsed esophagus can be seen.

(5/) Using a phased array probe you gain depth at the expense of resolution. Find what works for you.

(6/) Real time US of the trachea.
(7/) So now that we have familiarized ourselves with the ultrasonographic appearance of the trachea and adjacent structures.
Step1. Rule out esophageal intubations!!! With the ET tube in the esophagus you will see a double trachea or double tract sig
Step1. Rule out esophageal intubations!!! With the ET tube in the esophagus you will see a double trachea or double tract sig

(8/) ** Double Barrel Trachea ** in esophageal intubation s

(9/) Step 2: Determine Lung sliding on the right. This indicated tracheal or endobronchial intubation. (works best in non-spontaneously breathing patients with delivery of breaths via bagging or the vent)
(10/) Step 3: Determine left lung sliding in a similar fashion. in no lung sliding then likely a right main stem intubation. Retract the ET tube slightly until lung sliding is demonstarted on the left. this indicates bilateral lung ventilation!
(11/) Below is an example of no lung sliding on the left. What you do you see is the "Lung Pulse"! Don't let that shimmering effect fool you. It represents the transmission of the heart pulsations to the pleural line and is pathognomonic for lung collapse. See Lichtenstein et al.
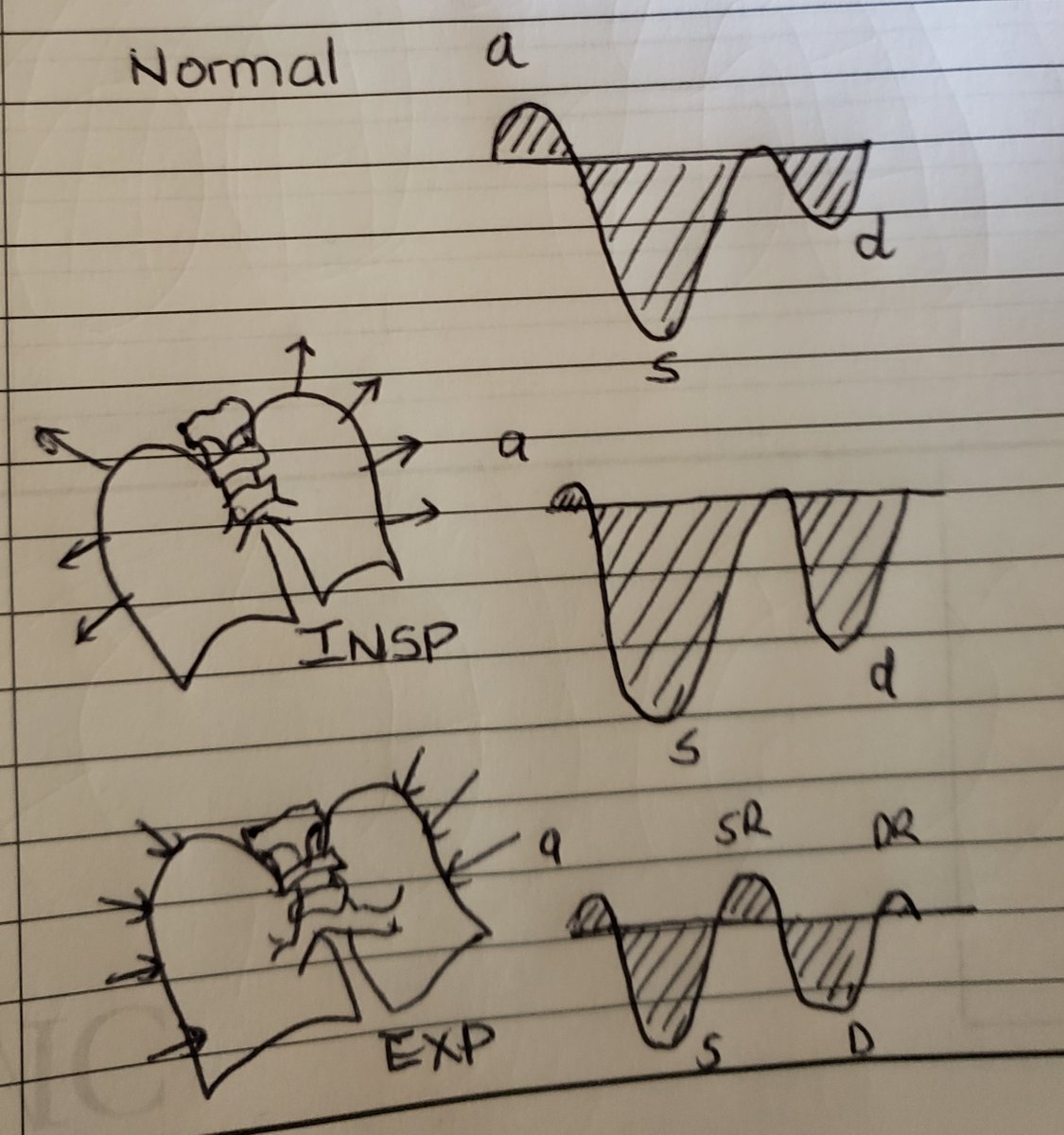
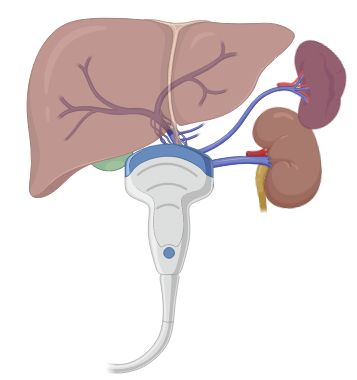
(12/) In equivocal cases Diaphragmatic Ultrasound can be utilized either by looking at diaphragmatic movements from the subcostal view of the area of interest or looking at the PLAPs point for lung curtain sign!
(13/) Caveats
- This protocol depends on the ability to detect bilateral lung vent via lung sliding therefore preexisting conditions that affect the pleural line may limit this. Pre-scan is preferred. Many things can cause a lack lung sliding!
- This protocol depends on the ability to detect bilateral lung vent via lung sliding therefore preexisting conditions that affect the pleural line may limit this. Pre-scan is preferred. Many things can cause a lack lung sliding!

(14/) This protocolized, systematic approach using tracheal and thoracic ultrasonography can be used to confirm endotracheal intubation, detect main stem intubations, and adjust tube positioning in the critically ill.
(15/) This has the potential to be used for routine intensive care, out-of-hospital or resource-poor settings, or situations which require isolation precautions to mitigate the use of CXR. So grab those probes and give it a try.

@Phani_kc @pdsalinas @ArgaizR @iceman_ex @ThinkingCC @kyliebaker888 @Pocus101 @IM_POCUS @drmarcogarrone @PulmCrit @BCM_Lung @bcmhouston @CCF_IMCHIEFS @CCF_PCCM @LatifiMani @krveshi @POCUS_Society @pocusfoamed @POCUSAcademy @pocusmeded @PhilipsPOCUS @NephroP @UAB_Sono @PittIMPOCUS
@AIUMultrasound @HeyDrNik @MaizeandLube @ACEP_EUS @SCUFellowships @UltrasoundJelly @ultrasound @CriticalCareNow @critconcepts @PittCCM @SCCM @IM_Crit_ @critcareexplore @critconcepts @iBookCC @ICS_updates @I_C_N @intensiveblog @siddharth_dugar @msiuba @nsenussiMD @suzanskef
• • •
Missing some Tweet in this thread? You can try to
force a refresh