
Intensivist. Cardiologist. Lifelong martial artist. Hemodynamics, Shock & Resuscitation.
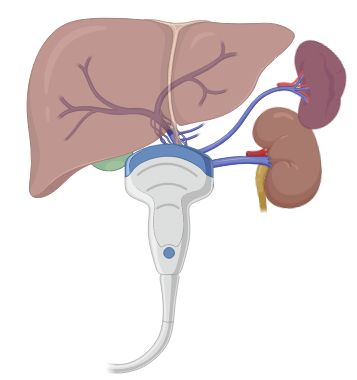
 Hepatic veins can provide a plethora of information on the "right heart apparatus".
Hepatic veins can provide a plethora of information on the "right heart apparatus".  Alternatively can use the back end of specially designed needles that obviate the need to remove your syringe from the needle. I find it more cumbersome but allows for aspiration of blood!
Alternatively can use the back end of specially designed needles that obviate the need to remove your syringe from the needle. I find it more cumbersome but allows for aspiration of blood! 



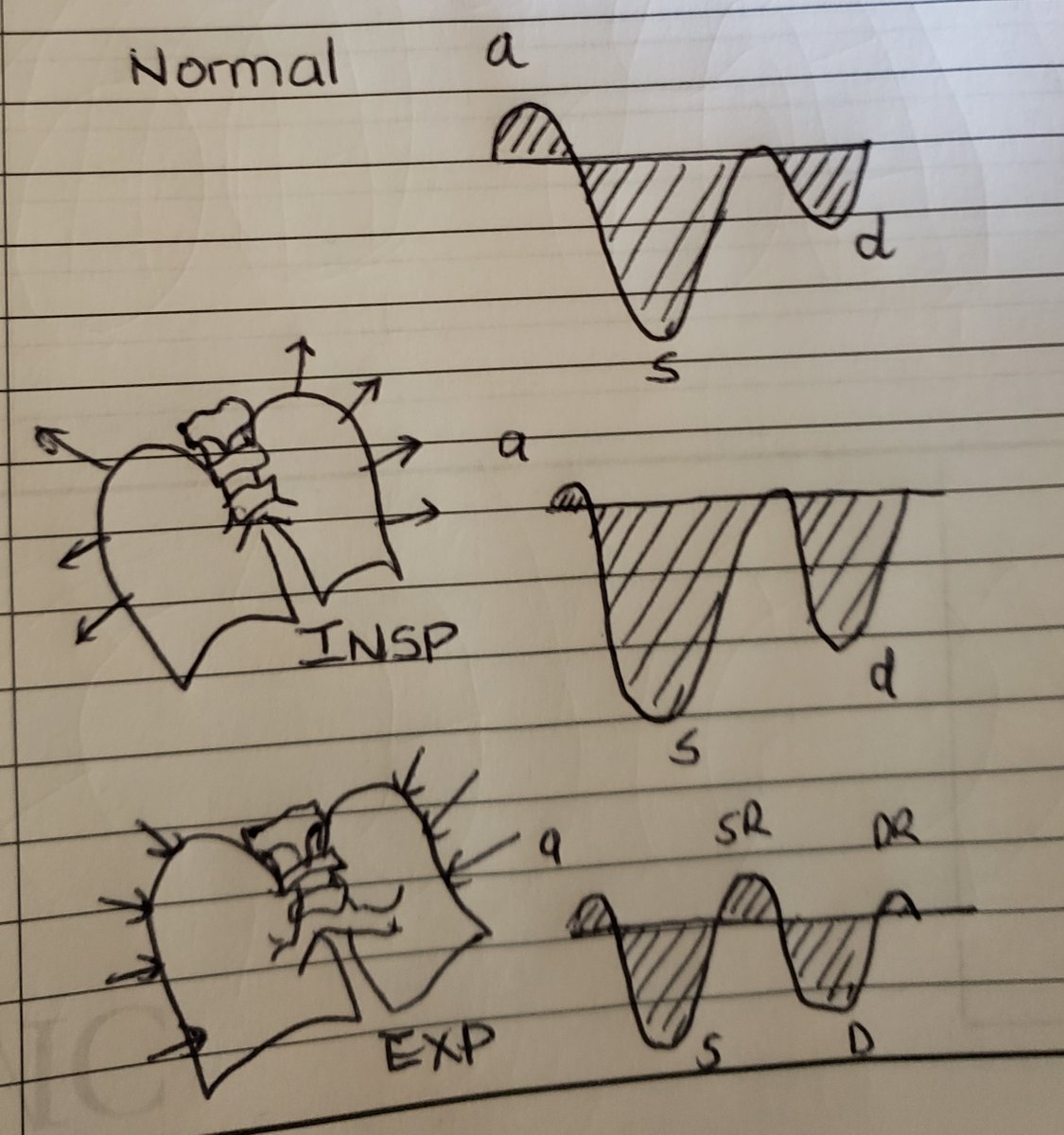
 ...a thorough understanding of these waveforms, hemodynamic correlates, and dynamic changes that occur in physiology and disease, is paramount to incorporating this into practice. #shocksquad #tweetorial #VEXUS #showmethewaveform. Here are rules of interpreting hepatic waveforms
...a thorough understanding of these waveforms, hemodynamic correlates, and dynamic changes that occur in physiology and disease, is paramount to incorporating this into practice. #shocksquad #tweetorial #VEXUS #showmethewaveform. Here are rules of interpreting hepatic waveforms
