live tweeting: "Time's Up: Eliminating Sexual Harassment & Gender Inequity in Healthcare" by @SharonneHayes 



Women may have different leadership styles than men. Countries led by women have had fewer issues with COVID-19 🔥
-@SharonneHayes
-@SharonneHayes


The fact that this was published, in multiple editions, proves that more women need to be involved in publishing.
-@SharonneHayes
-@SharonneHayes

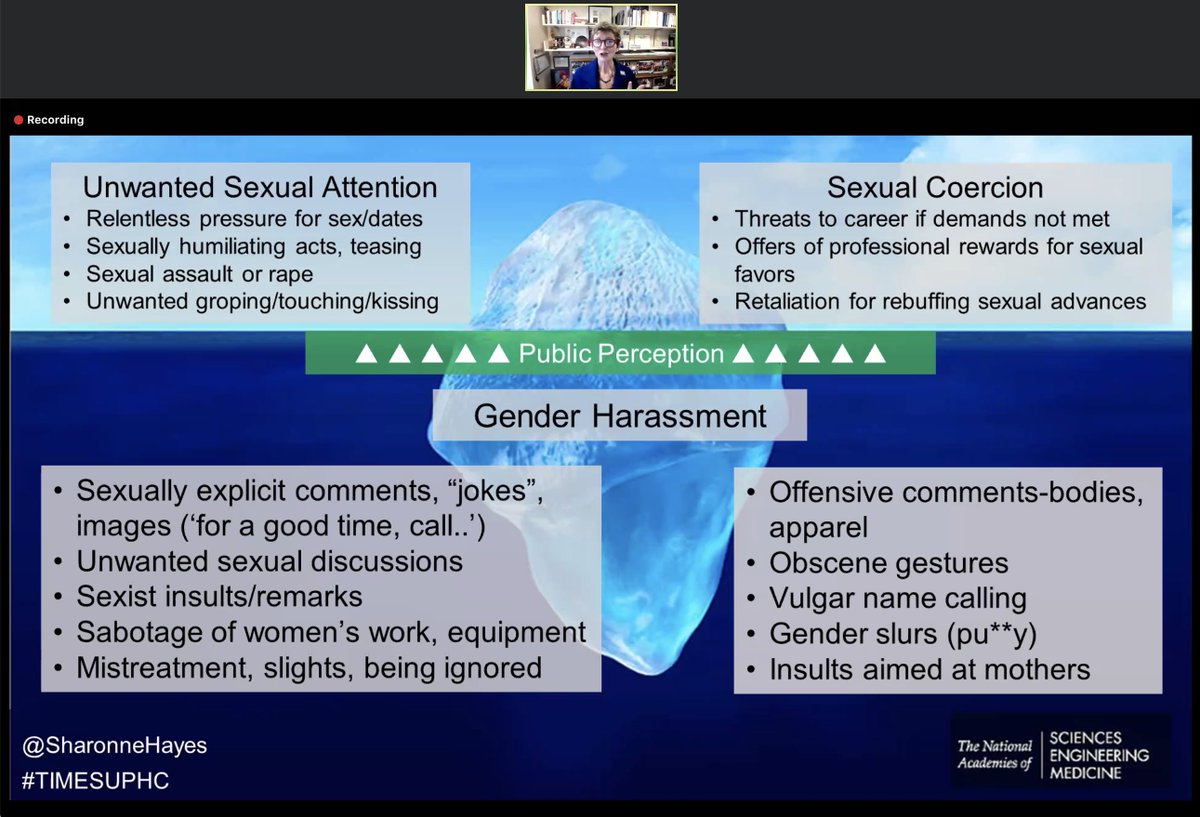
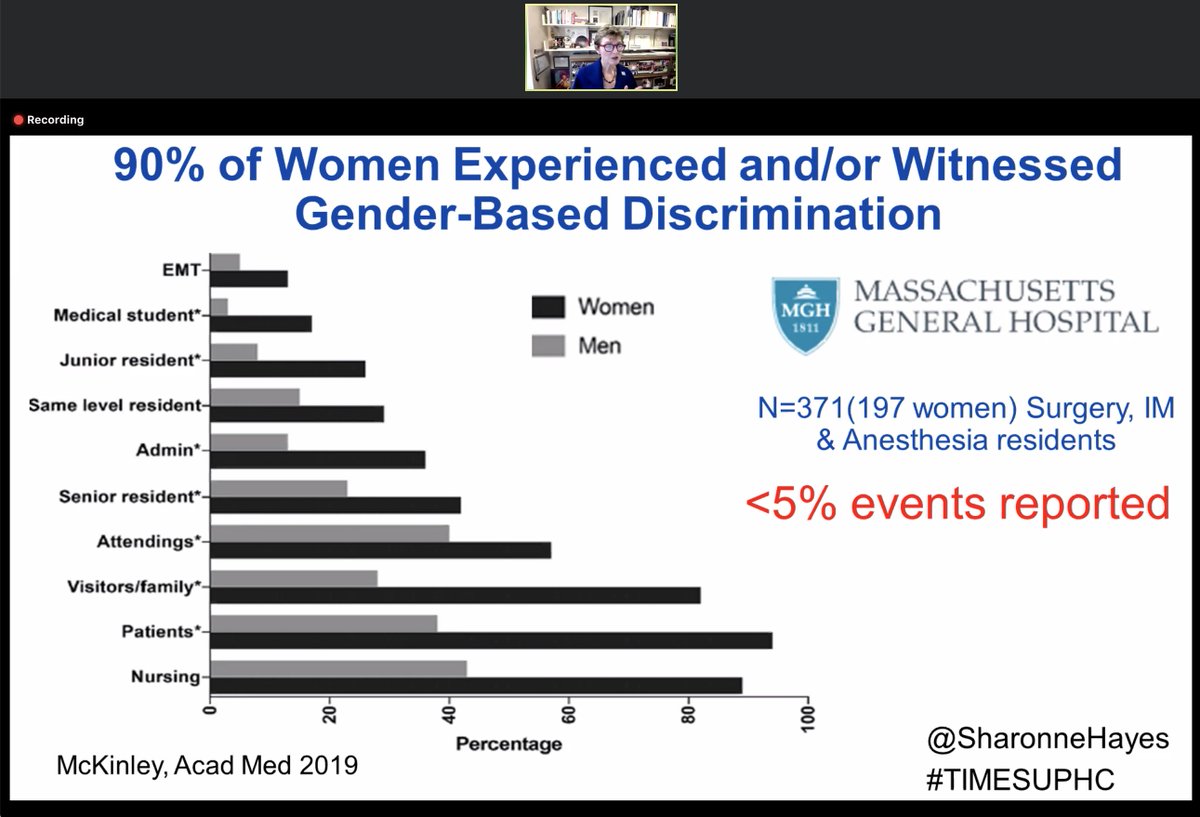
Busting Myth #1: Sexual harassment doesn't just happen to a few women - it's pervasive. And generally unreported.
-@SharonneHayes
-@SharonneHayes

Busting myth #2: It's not just a few "bad apples." Rather, organizational climates allow harassment ("structural sexism"?)
-@SharonneHayes
-@SharonneHayes

Busting myth #3: The impact is very real, in multiple dimensions. Sexual harassment is a severe occupational hazard which (within the research realm) constitutes research misconduct (potentially meriting defunding researchers).
-@SharonneHayes
-@SharonneHayes



Policies and training can help staff deal with sexual harassment. Good intentions aren't enough. Centralizing processes within an organization can help as well.
-@SharonneHayes
-@SharonneHayes




Incidents should be investigated systematically. Implementing a system to deal with reporting at Mayo led to a temporary surge in reports. Internally *posting* data changed the institutional culture, by demonstrating that incidents were taken seriously.
-@SharonneHayes
-@SharonneHayes



Most reports were substantiated, largely relating to male physicians in positions of power. Mayo is tracking out sexual harassment the way everyone else is tracking COVID.
-@SharonneHayes
-@SharonneHayes


Harassment is a marker for other dimensions of inequity (e.g. under-representation in leadership).
-@SharonneHayes
-@SharonneHayes


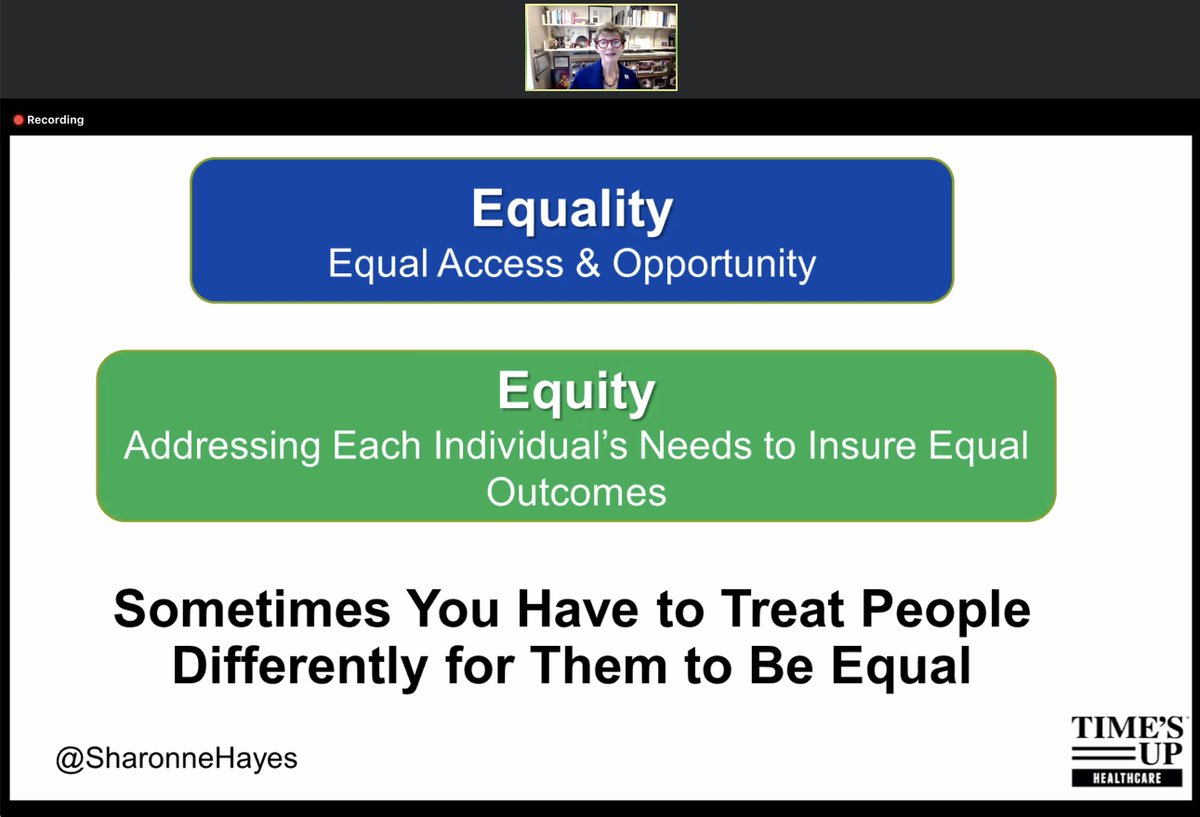
*Equity* is analogous to tailoring heart failure therapy specific to different genders. Alternatively, *equality* would involve treating every patient exactly the same way.
-@SharonneHayes
-@SharonneHayes








We have a long ways to go. (My apologies for barely scratching the surface of this incredible talk)
#RBGForever
#RBGForever




• • •
Missing some Tweet in this thread? You can try to
force a refresh