
🚨BIG NEWS: In January, the unpublished VICTAS trial of vitamin C in #sepsis was stopped after enrolling just 501 of a planned 2000
Now data on clinicaltrials.gov shows why, and it doesn’t look good for #vitaminC. Is this the last🔩in⚰️of the ‘metabolic cure’?
A short🧵
1/
Now data on clinicaltrials.gov shows why, and it doesn’t look good for #vitaminC. Is this the last🔩in⚰️of the ‘metabolic cure’?
A short🧵
1/
I’ve been hopeful but more than a little skeptical about the 🍹🍋 metabolic cocktail for sepsis (vitamin C + hydrocortisone + thiamine) since the original before/after case series.
I’ve followed this literature closely & have been waiting eagerly for the results of the RCTs.
2/
I’ve followed this literature closely & have been waiting eagerly for the results of the RCTs.
2/
Thats’s why I was excited to see that VICTAS had posted results. bit.ly/3j3Iatl
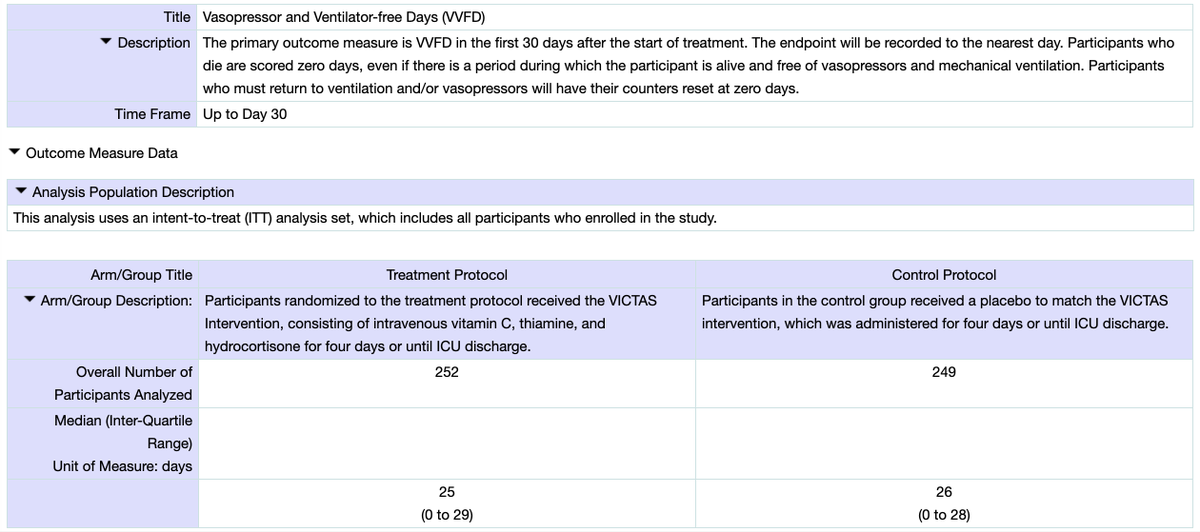
The VICTAS trial is the largest (& arguably best) of the vitamin C RCTs: a placebo-controlled, Double-blind RCT done at 43 sites across the US. The 1° endpoint was vasopressor free days.
3/
The VICTAS trial is the largest (& arguably best) of the vitamin C RCTs: a placebo-controlled, Double-blind RCT done at 43 sites across the US. The 1° endpoint was vasopressor free days.
3/
The results are incomplete & we will need to wait for the actual publication to get the full picture.
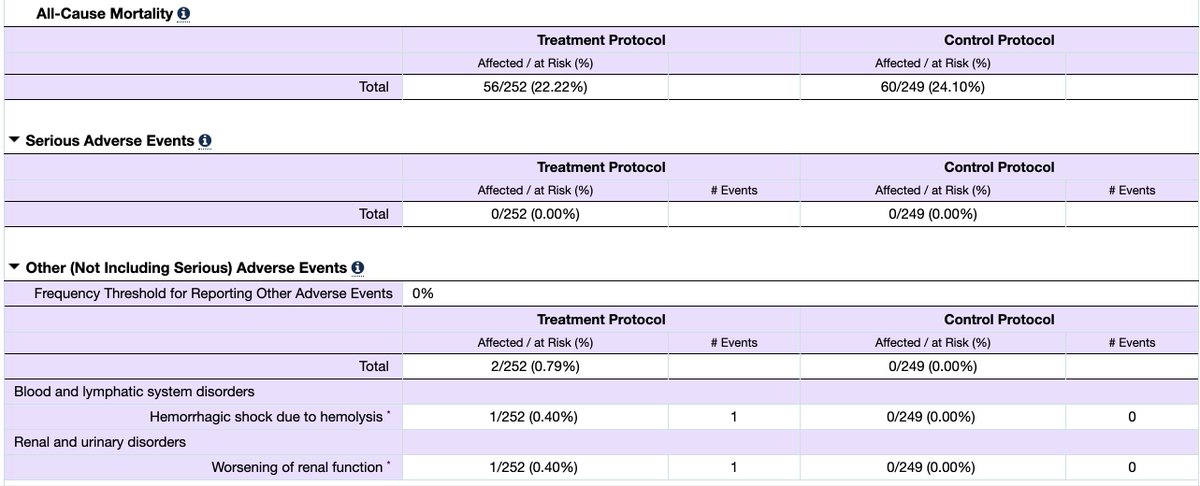
But what we can see doesn’t look good:
* similar mortality rate in both arms
* more vasopressor free days in the control group
* some adverse events in the vitamin C arm
4/
But what we can see doesn’t look good:
* similar mortality rate in both arms
* more vasopressor free days in the control group
* some adverse events in the vitamin C arm
4/
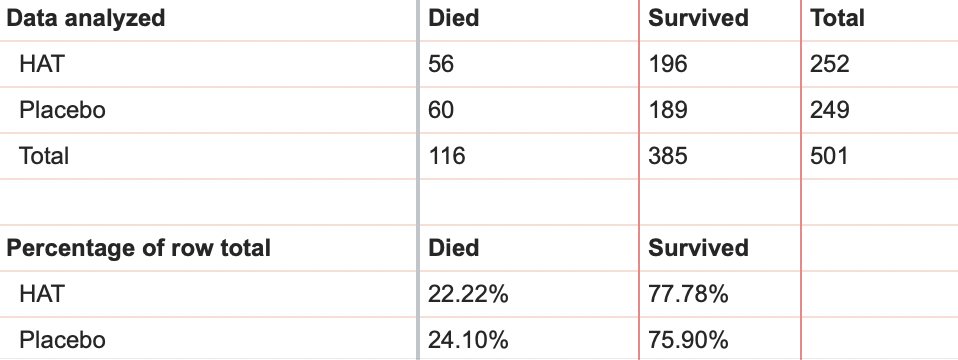
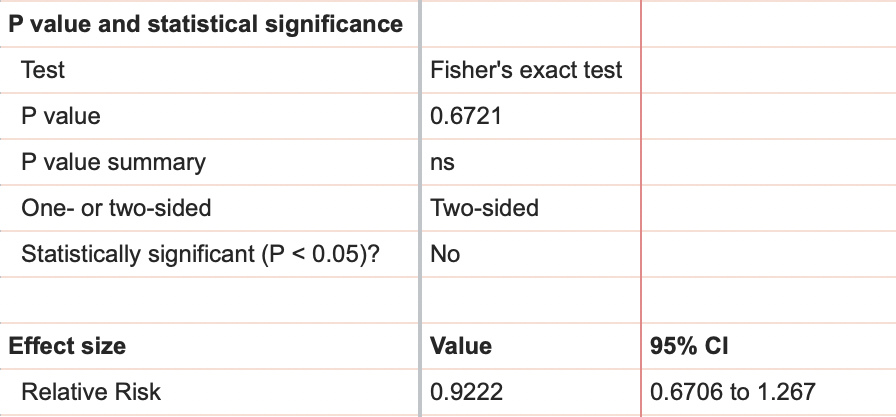
Even with this limited data and some simple stats, we can see that there is no significant difference in all cause mortality:
- HAT 22.2% vs Placebo 24.1% (RR 0.92 95% CI 0.67 - 1.27; p = 0.67)
There also isn’t a difference in vasopressor free days:
- HAT 25 vs Placebo 26
5/
- HAT 22.2% vs Placebo 24.1% (RR 0.92 95% CI 0.67 - 1.27; p = 0.67)
There also isn’t a difference in vasopressor free days:
- HAT 25 vs Placebo 26
5/
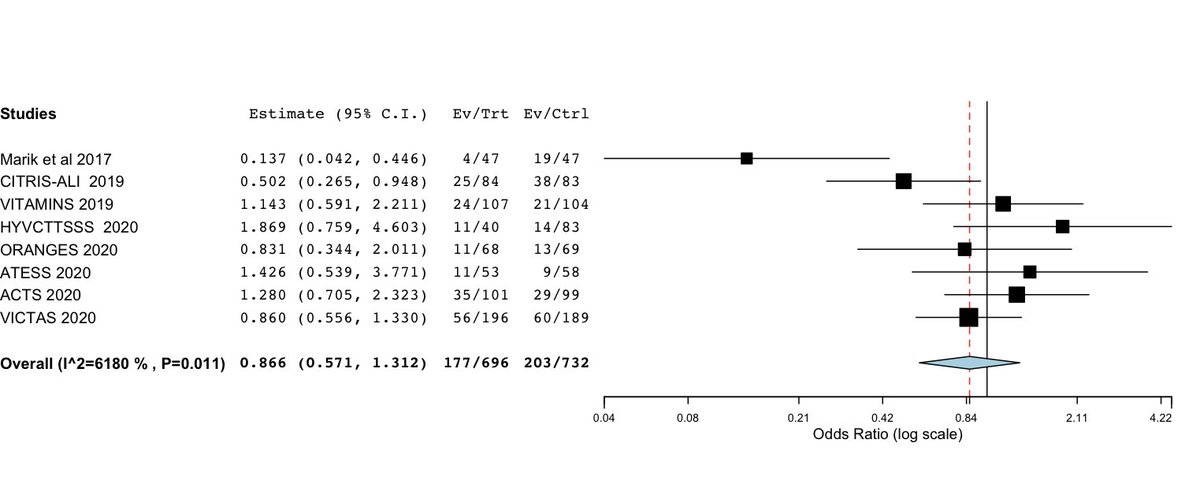
When we think about these results in the context of the other published studies it 🎨a consistent🖼:
- *not one* study has replicated the effect seen by Marik et al
See my updated Forrest Plot (full blog post soon): The more studies we do the smaller the overall effect.
6/
- *not one* study has replicated the effect seen by Marik et al
See my updated Forrest Plot (full blog post soon): The more studies we do the smaller the overall effect.
6/
• • •
Missing some Tweet in this thread? You can try to
force a refresh
































