
The key to better control of the #covid19 pandemic may be in identifying & preventing #superspreading, through backward tracing to identify clusters. Need to rethink our approach.
Good article by @zeynep explaining the rationale.
theatlantic.com/health/archive…
Good article by @zeynep explaining the rationale.
theatlantic.com/health/archive…
Contact tracing seeks out where the infection has come from (look for source) & where it is going (contacts of the index who may be susceptible). An assumption is that all infections are equal (i.e. every infected person has a similar chance of infecting someone else).
1/n
1/n
So with COVID19, we assume with R0=2.6, 1 infected person infects 2.6 others. But this is an erroneous assumption if superspreading is a key mode of transmission. Some infected persons are more infective!
2/n
2/n

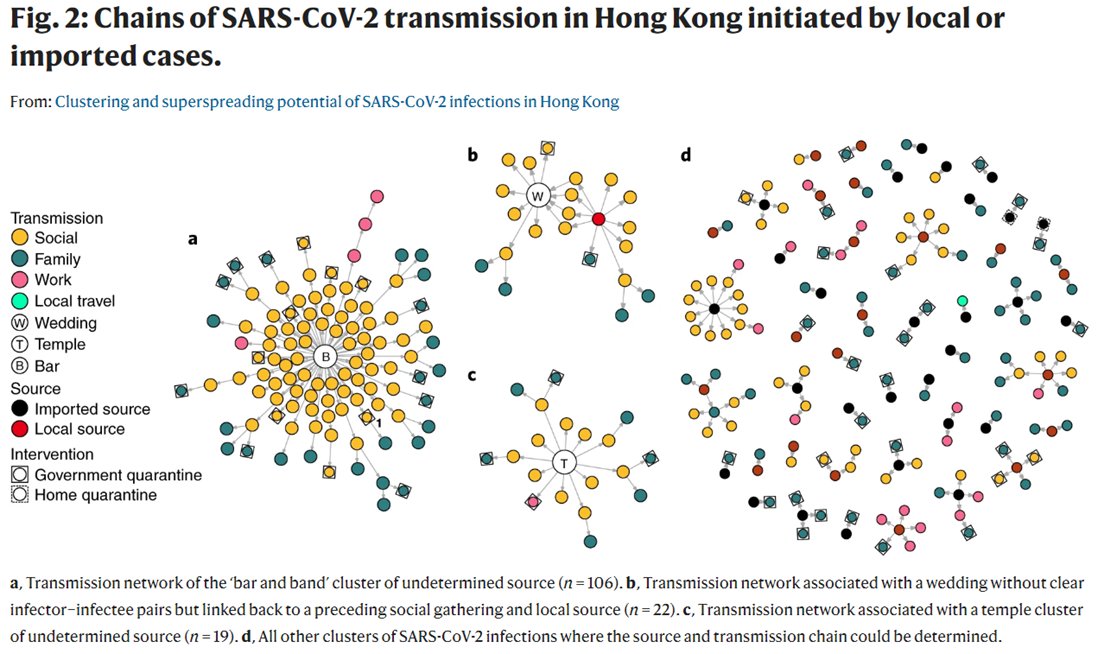
It has been evident that superspreading occurs in COVID19
80% of infections come from 20% of cases. In around 70% of cases, they don't infect anyone else.
3/n
80% of infections come from 20% of cases. In around 70% of cases, they don't infect anyone else.
3/n

This figure from an article in nature beautifully illustrates this dichotomy between superspreading and isolated cases
Source: nature.com/articles/s4159…
4/n
Source: nature.com/articles/s4159…
4/n
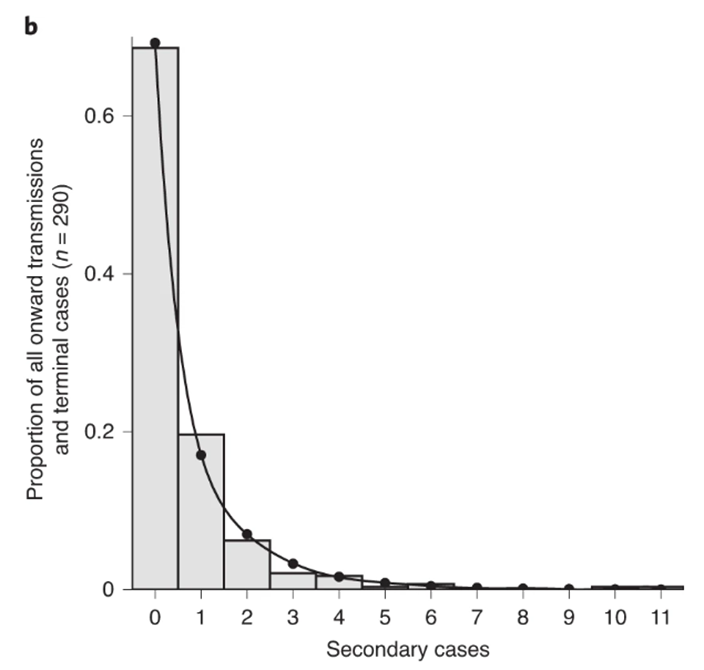
From the same paper they report this skewed distribution of proportion of onward transmissions. So most cases infect 0-1 others, but a tiny proportion infect many.
5/n
5/n
Likewise, this case report of a superspreading event in Ohio demonstrates this same phenomenon.
HT
6/n
HT
https://twitter.com/ScottGottliebMD/status/1293655055581749248
6/n

So if we only looked for onward (forward) transmission from the index we would be missing other infections and it would be low yield effort. If we included backward tracing to find the source who is more likely to be a superspreader we could uncover more chains of infection.
7/n
7/n


Hence their emphasis on backward tracing.
HT to @AdamJKucharski who tweeted this back in August
HT to @AdamJKucharski who tweeted this back in August
https://twitter.com/AdamJKucharski/status/1293472353758871552

The other useful suggestion in @zeynep article is the proposition that the lower sensitivity but high specificity tests could be deployed to help guide quarantine decisions. These tests may miss "true positives", but are unlikely to miss "true negatives".
10/n
10/n
So if you test a cohort of contacts, & they are all negative, highly unlikely there are cases there. But if you get a single positive, then chances are there are more cases in that cohort. This approach could be useful e.g. testing care homes, healthcare, education settings.
11/n
11/n
Final thought: I'm not convinced of the evidence for a blunderbuss approach to mass testing. It risks consuming much resource & is a distraction. Far more value in deploying finite test resources to uncover these clusters to target quarantine/isolation to stop transmission.
• • •
Missing some Tweet in this thread? You can try to
force a refresh






