
THREAD: what happened with COVID in September and where are we now? It's been an eventful month and there is good news and bad news... read on to find out which is which!
NB: Longish thread (18 tweets) but hopefully informative with lots of pretty charts...
@IndependentSage
NB: Longish thread (18 tweets) but hopefully informative with lots of pretty charts...
@IndependentSage
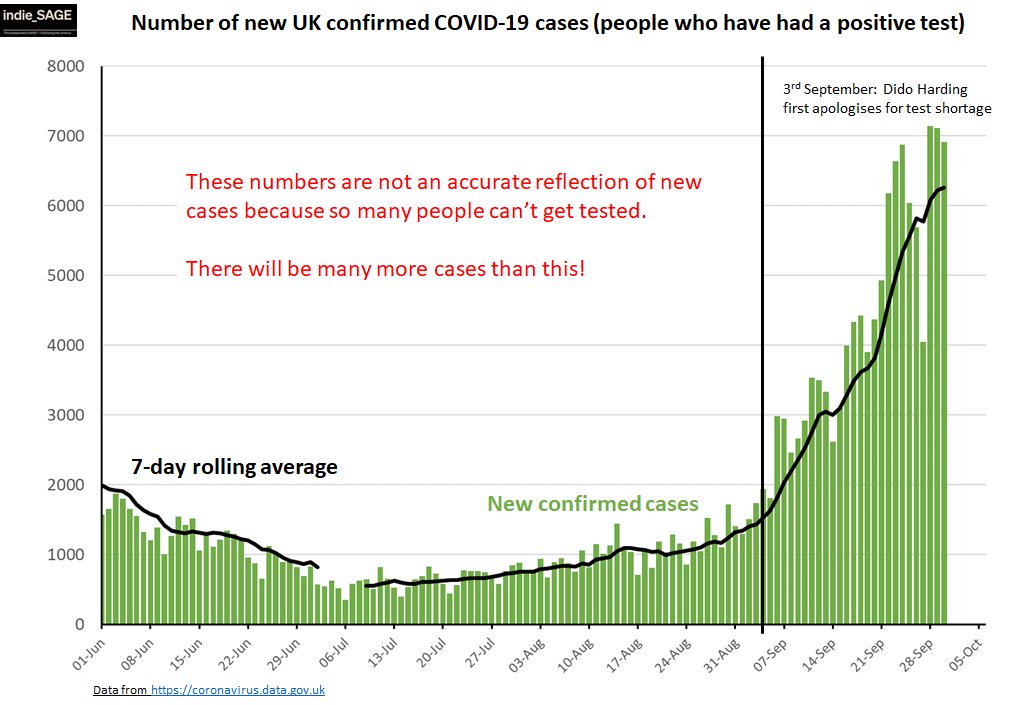
Confirmed cases have continued to rise, but hard to interpret cos of ongoing problems with testing. But let's go with this for now - where are the confirmed cases? 
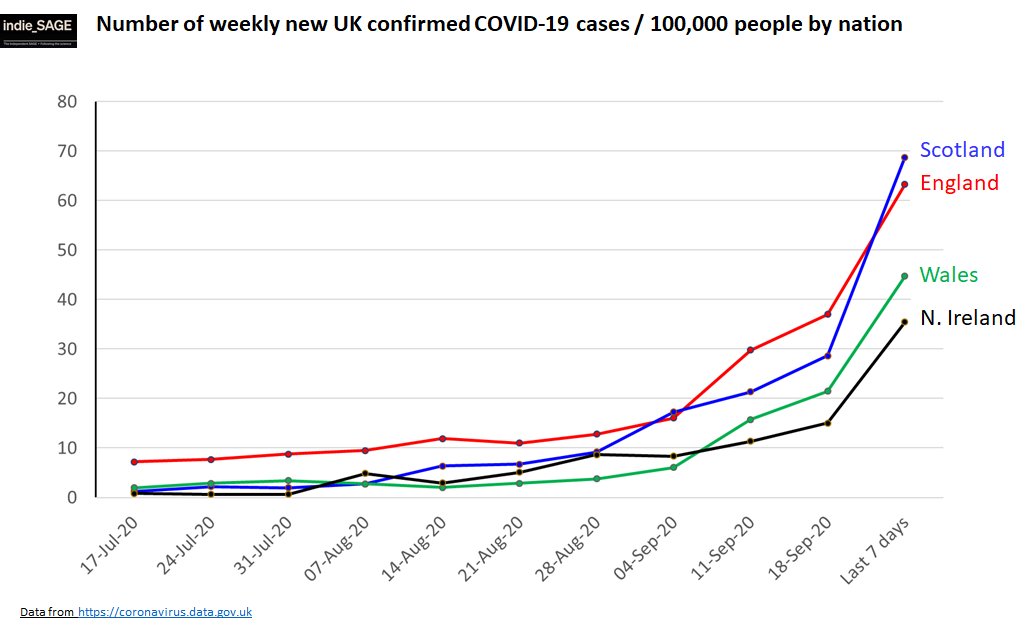
All the nations have seen steep increases over September but Wales and N Ireland doing rising less steeply than England and Scotland... Let's dig a bit further into England
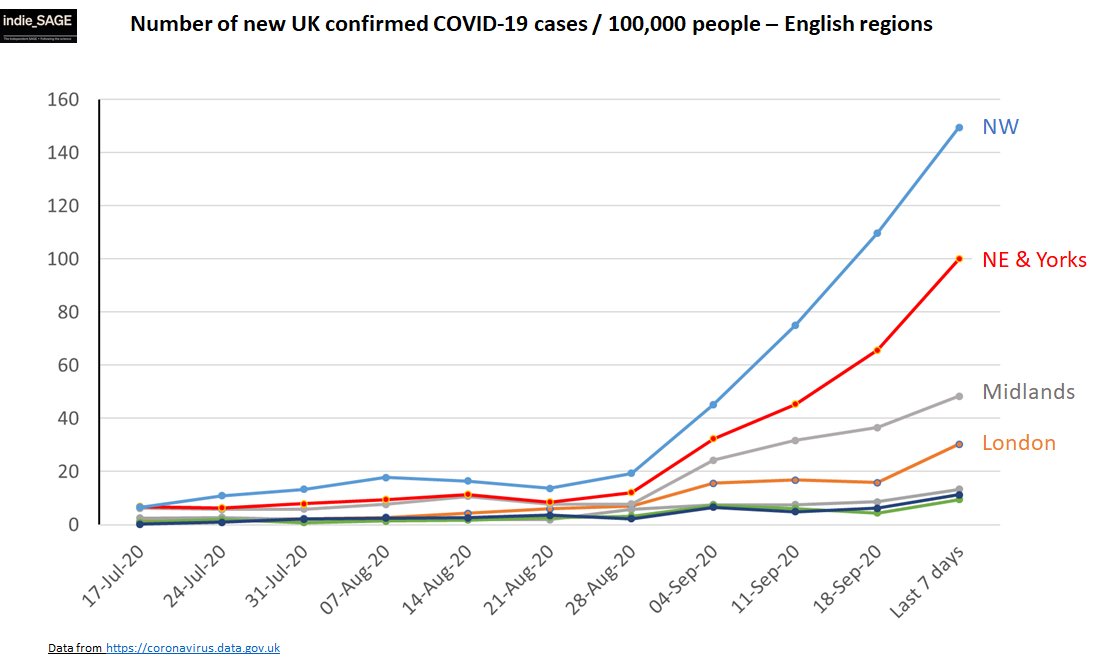
Big regional variation. Cases rising fastest in NW, NE, Yorks & Humber. Then Midlands and London... From confirmed cases look like there are 3 epidemics at least in England. The increase in cases has not surprisingly led to increase in hospitalisations
And hospital admissions are regionally different too - NE+Yorks, NW saw big increases over Sept (and continuing increases). Midlands + London increased but have recently plateaued... Rest of country not seeing big rises.

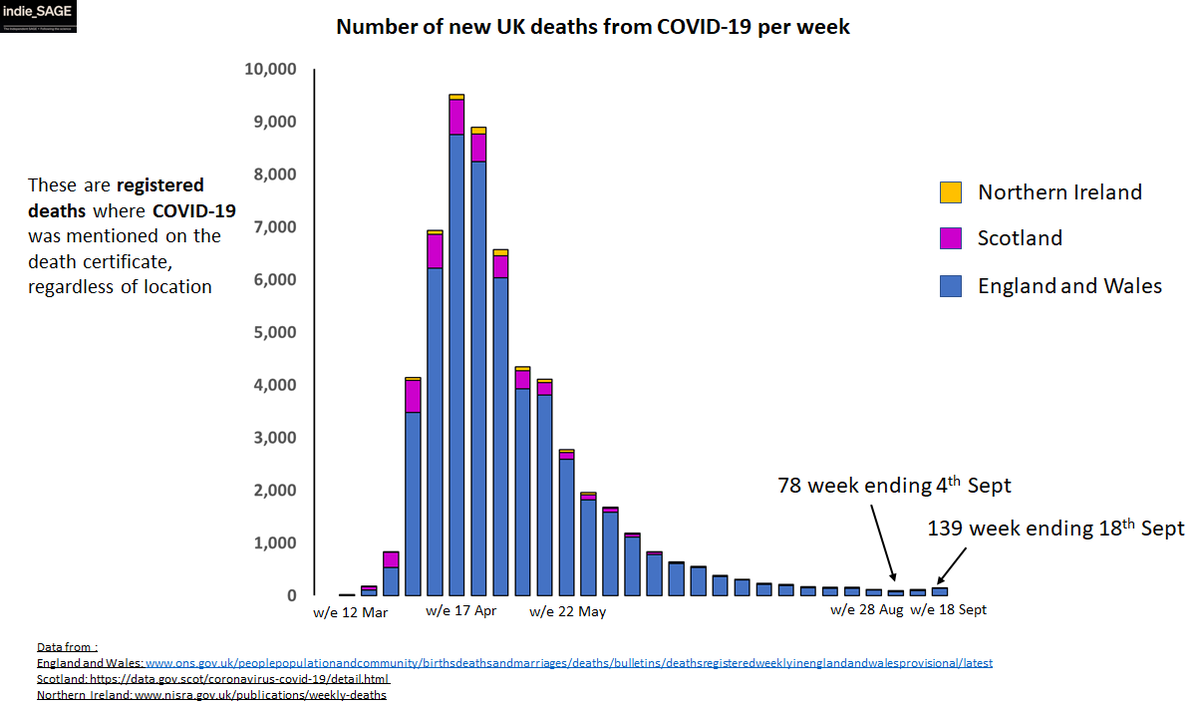
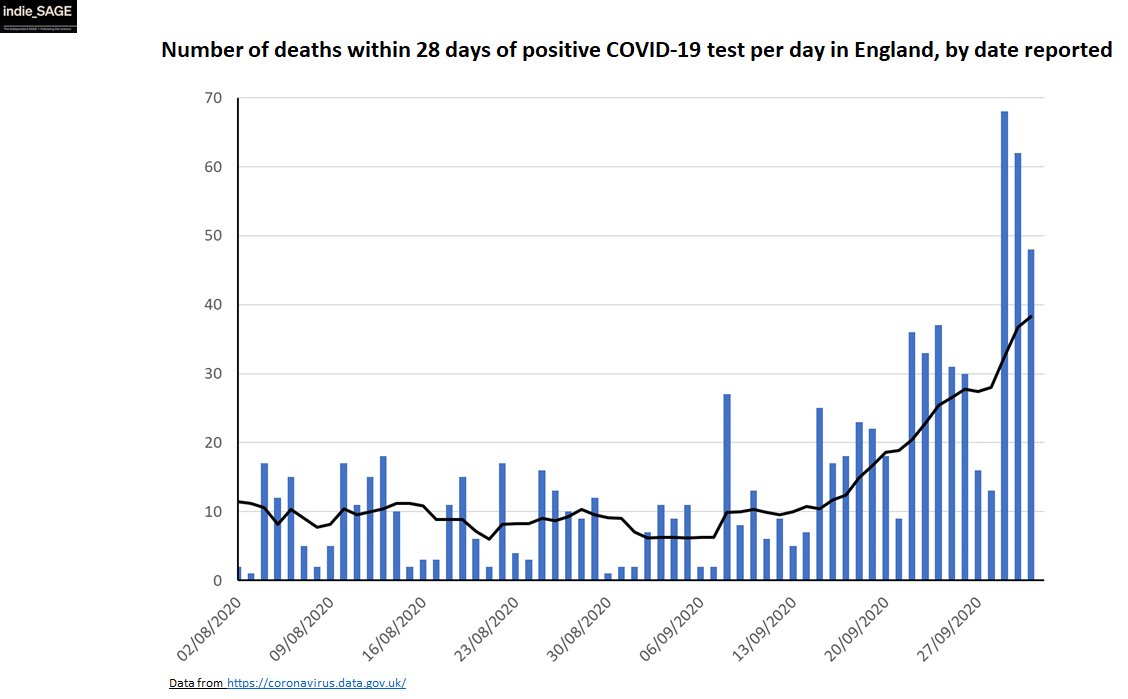
Unfortunately, increasing hospital admissions lead to increasing numbers of deaths a few weeks later, and we are now seeing this: in both ONS death registry data (gold standard) & daily deaths within 28 days of a +ve test. While hospital admissions stay high, this will continue.
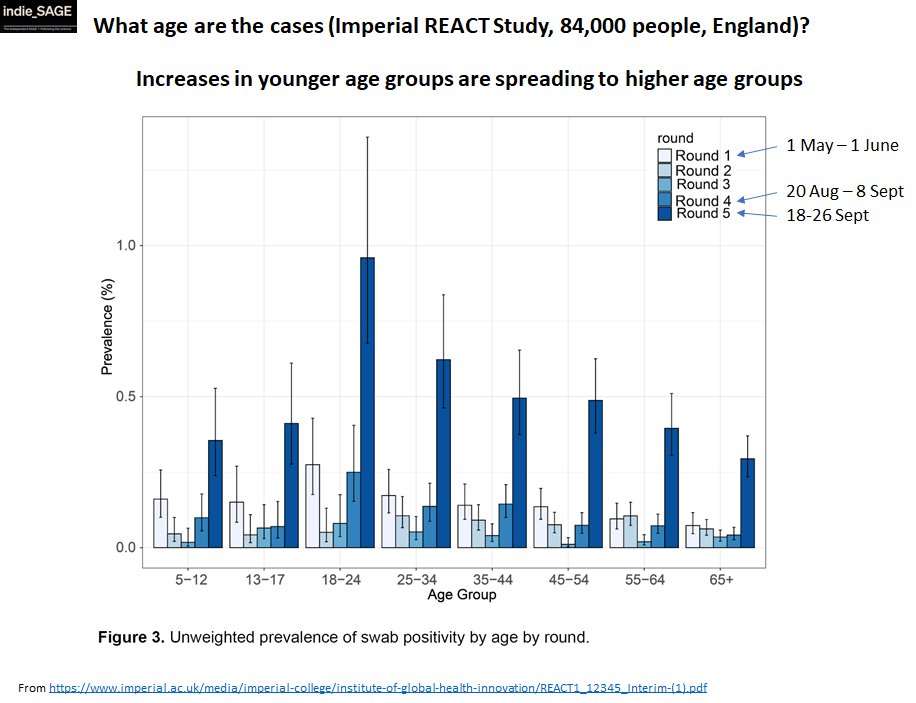
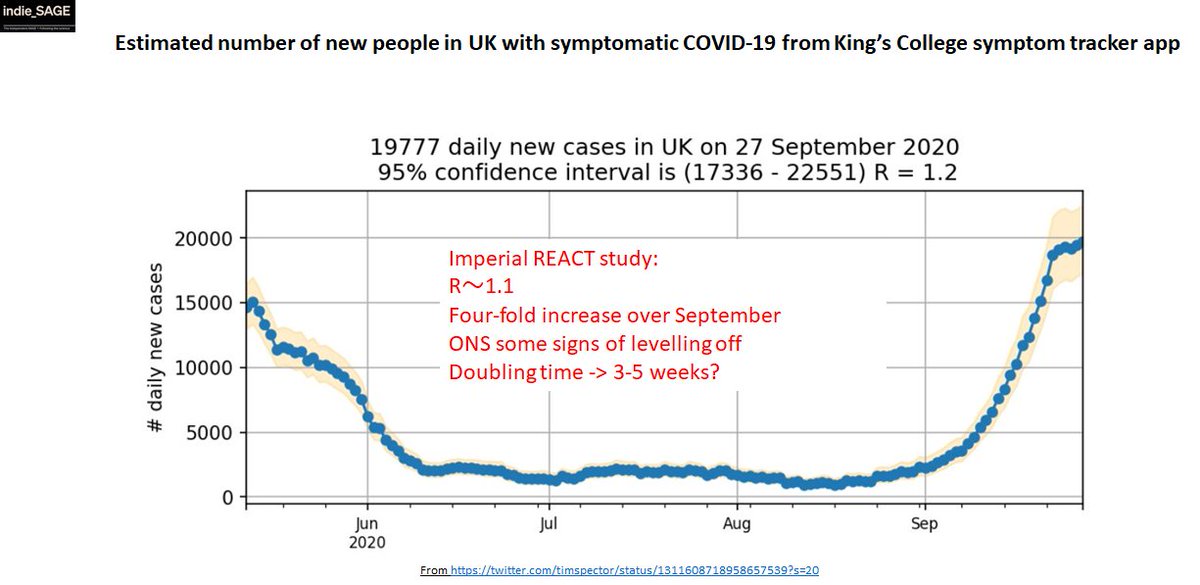
Ok, so moving on from confirmed cases, let's look at interim results from @imperialcollege REACT study that published results from 84K randomly sampled people yesterday - gives a much better picture of detail & extent of spread. imperial.ac.uk/news/205473/la…
1) fourfold increase in cases over September - there is a LOT more virus around now. Concentrated in 17-24 yr olds but fastest growth in 65+ (worrying for future hosp admissions). Under 16s don't seem more infected than rest - schools don't seem to be increasing transmission
Also worrying that the BME population twice as likely to have COVID, esp given known to be more at risk from severe disease (and already ICNARC says new ICU COVID patients disproportionately BME). Increased spread does not impact people evenly
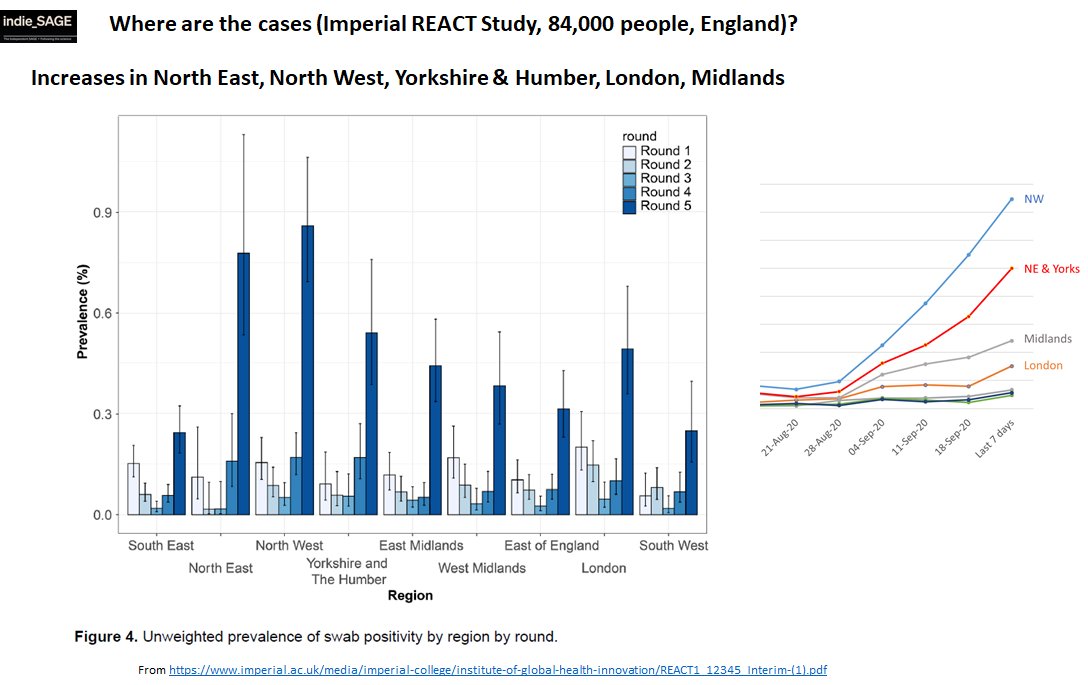
The geographic distribution is interesting. Yes NW, NE & Yorks still highest by a way, but London also very high (and HIGHER than Midlands). So, are the reduced London *confirmed* cases due to London not getting enough tests?
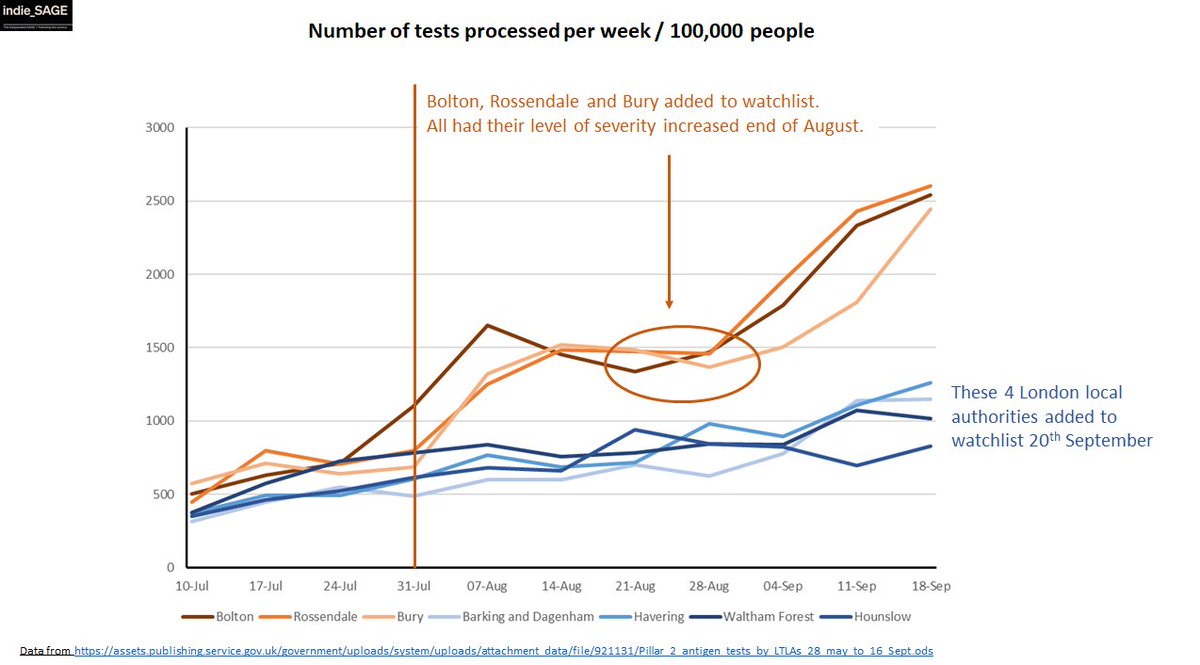
We can see here from comparing 3 LAs in the NW to 4 from London how being on the PHE watchlist does seem to trigger more testing - not a bad thing if there's plenty of capacity. When there isn't (like now), risks new hotspots being missed for a while (e.g. London)
Now for some good news.... Although we had very rapid and substantial spread in Sept, recent week seems to show slowing from KCL symptom app, REACT study and ONS. Doubling time likely to be 3-5 weeks which is a big improvement on 8 days a few weeks ago!
That said, overall R or doubling time probably not that helpful given to how differently epidemic is playing out in the North compared to Midlands & London and then SW & SE.
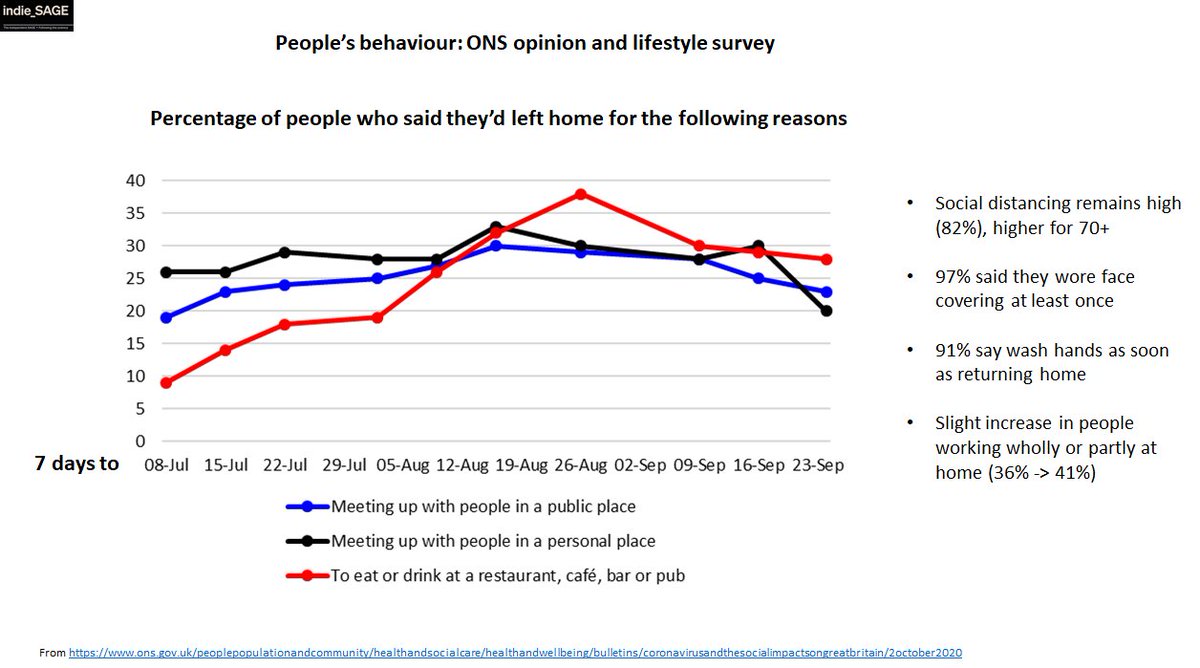
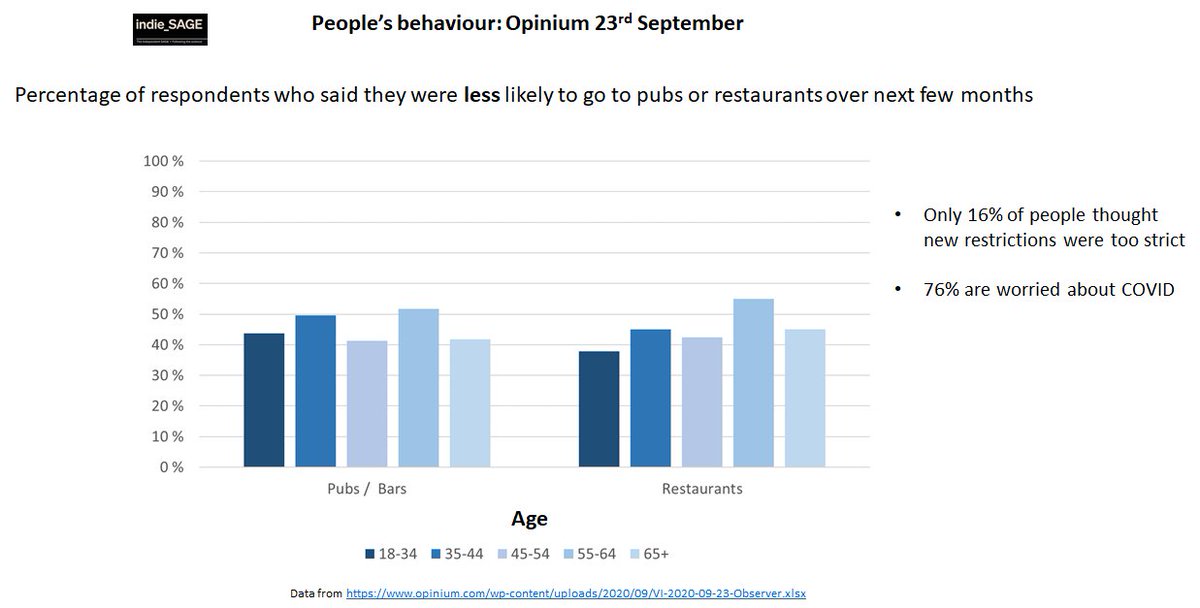
But slowing is slowing and what could be causing it? People are going out less now and intend to go out less in future. People ARE modifying their behaviour and support restrictions. Good news!
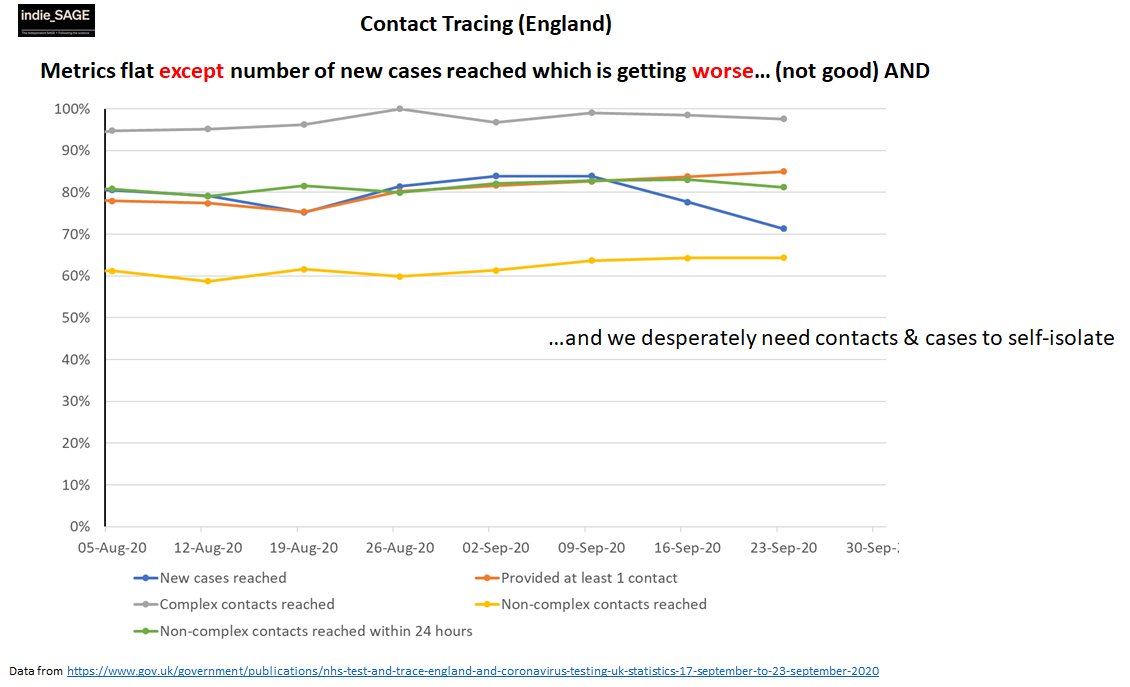
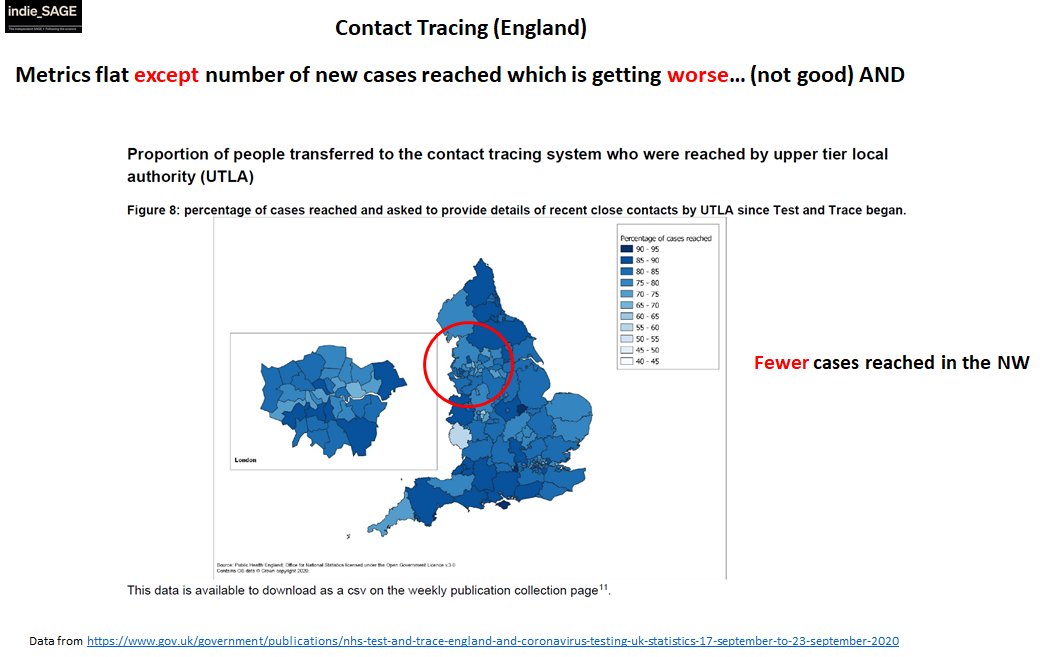
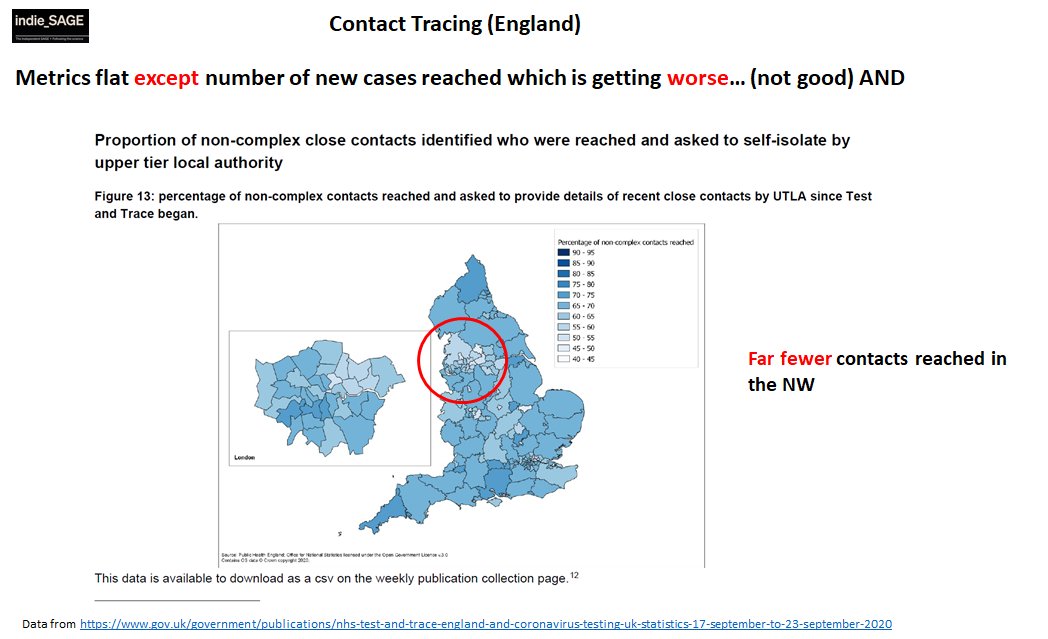
Meanwhile contact tracing (remember that? the way out of restrictions? the thing govt is meant to be fixing?) is not doing so well... New referred cases reached has dropped from 82% to 71% recently, little else improving. Still need support for isolation.
Even more concerning, it is performing WORST where it is needed the MOST (NW). This might partly expain why growth in NW is more rapid than elsewhere.
So where are we for October? Well it's a tale of the good, the bad and the ugly...
GOOD: growth is slowing quite a bit. We've bought ourselves a lot more time.
BAD: Massive increase in COVID in Sept
UGLY: Contact tracing
GOOD: growth is slowing quite a bit. We've bought ourselves a lot more time.
BAD: Massive increase in COVID in Sept
UGLY: Contact tracing
LAST TWEET: What have we bought ourselves time for? What's the strategy? We need a GOOD test & trace system that works -> REVERSES growth AND will let us ease off the restrictions. It's our way out! Govt MUST urgently fix it. We're doing our bit, they must do theirs.
• • •
Missing some Tweet in this thread? You can try to
force a refresh






















