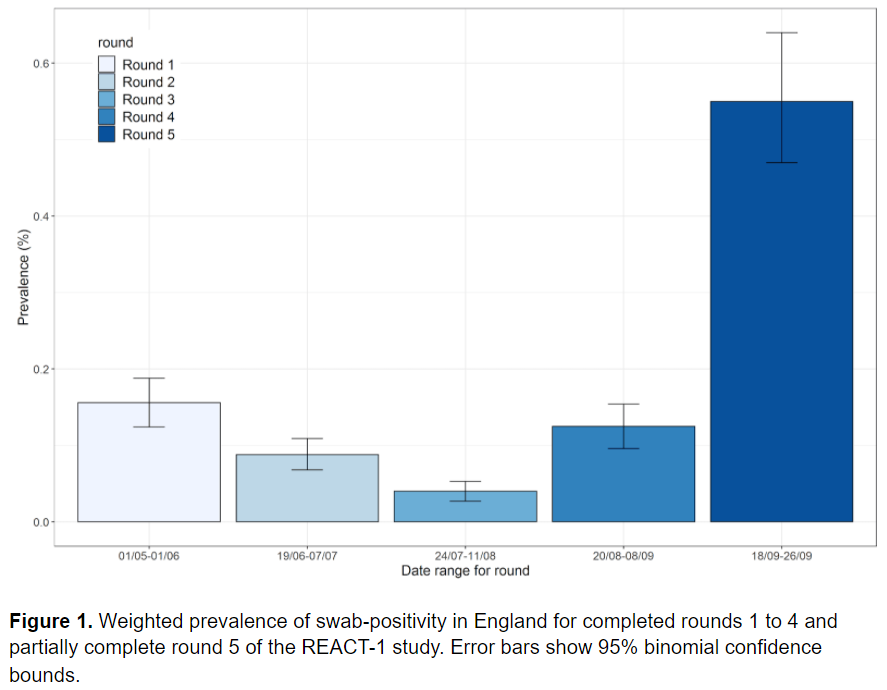
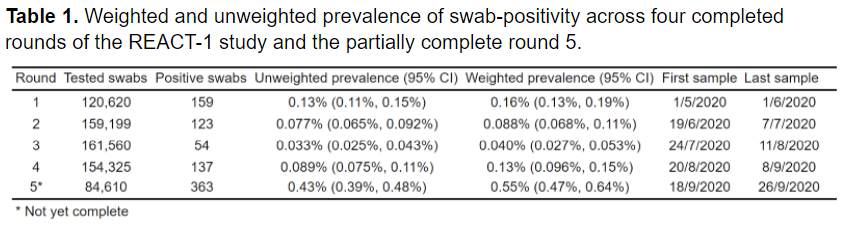
REACT-1 study update: Prevalence of swab positivity had increased to over 1 in 200 in England as of 26 Sep 2020. Weighted prev = 0.55% (0.47%, 0.64%). This implies 411,000 (351,000, 478,000) people are virus-positive.
Full results on medrxiv: medrxiv.org/content/10.110… (1/n)
Full results on medrxiv: medrxiv.org/content/10.110… (1/n)
Main results:
- 363 positives from 84,610 samples
- Weighted prev = 0.55% (0.47%, 0.64%)
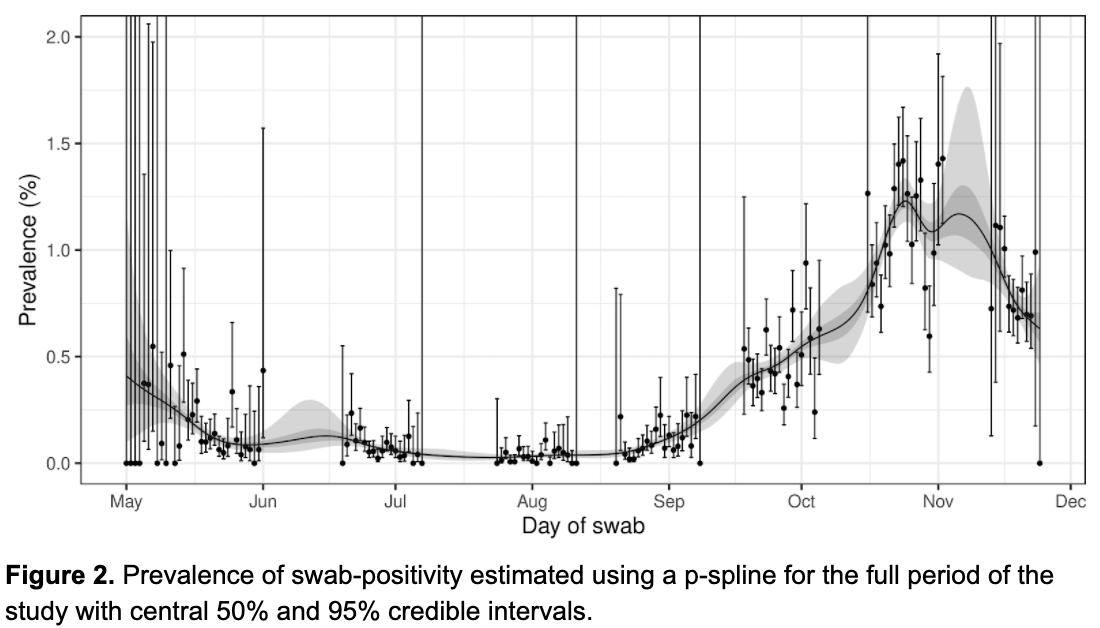
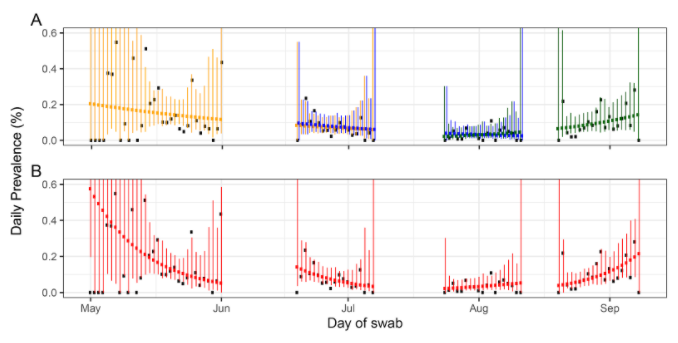
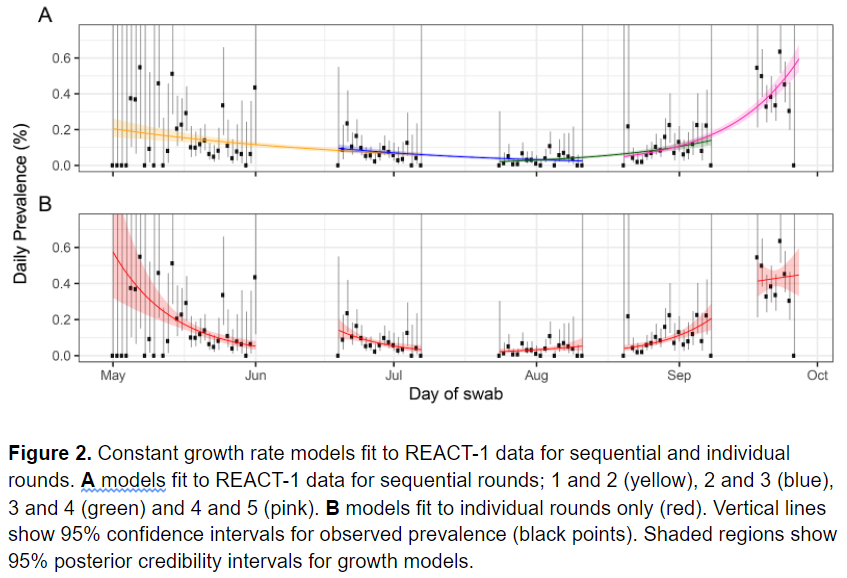
- This continues upwards trend in prevalence seen since mid-Aug
- Highest observed prev since beginning of study in May 2020 & more than a four-fold increase in weighted prev observed in r4
- 363 positives from 84,610 samples
- Weighted prev = 0.55% (0.47%, 0.64%)
- This continues upwards trend in prevalence seen since mid-Aug
- Highest observed prev since beginning of study in May 2020 & more than a four-fold increase in weighted prev observed in r4
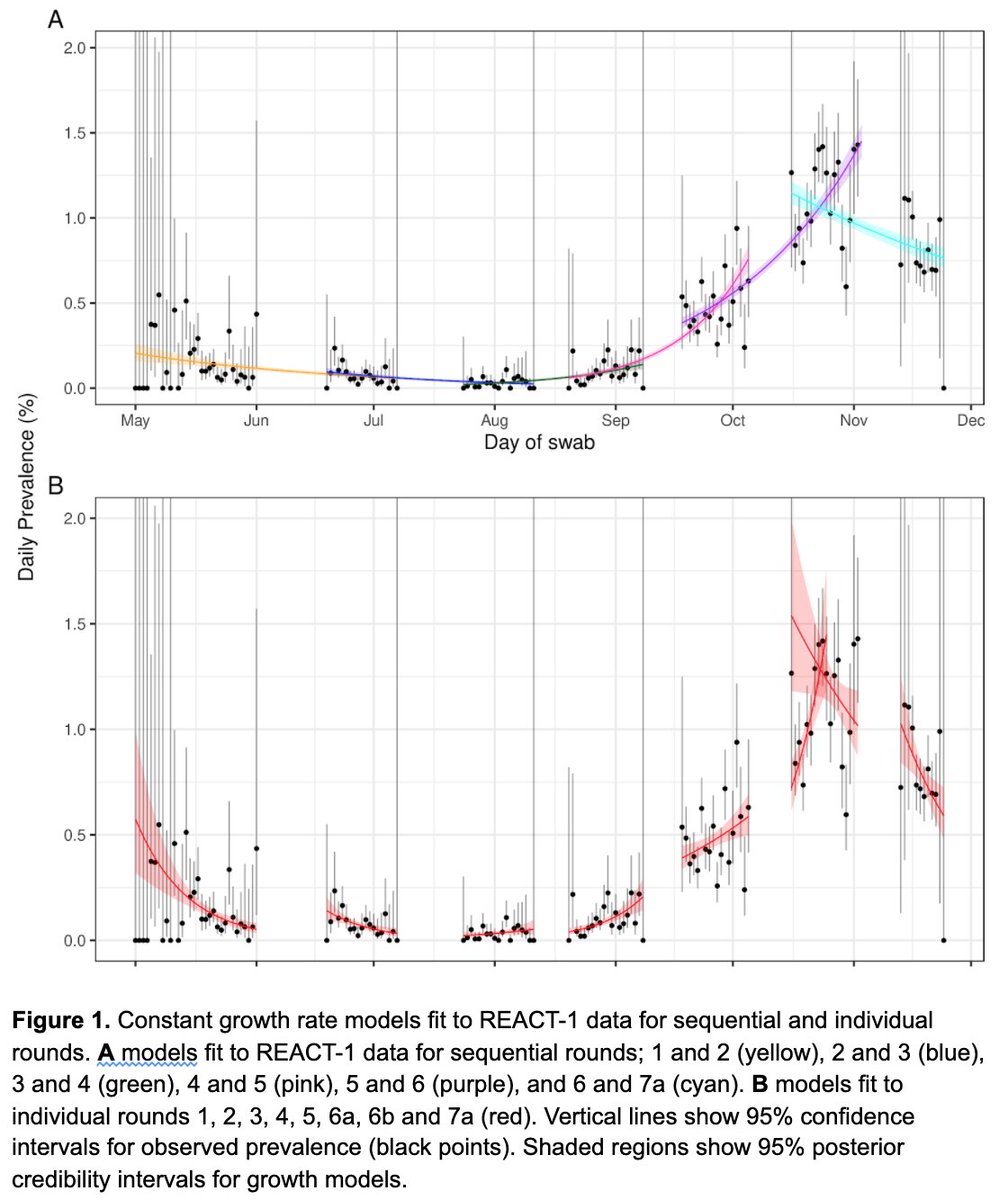
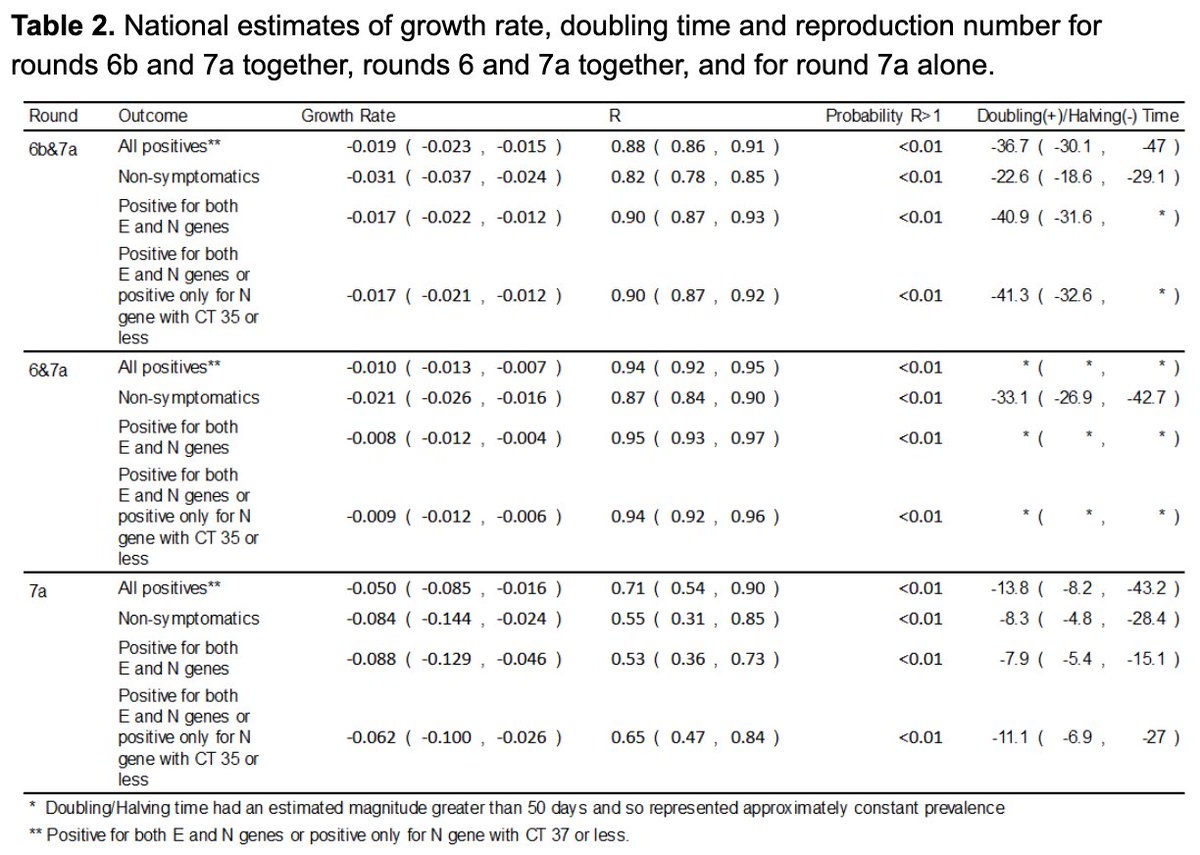
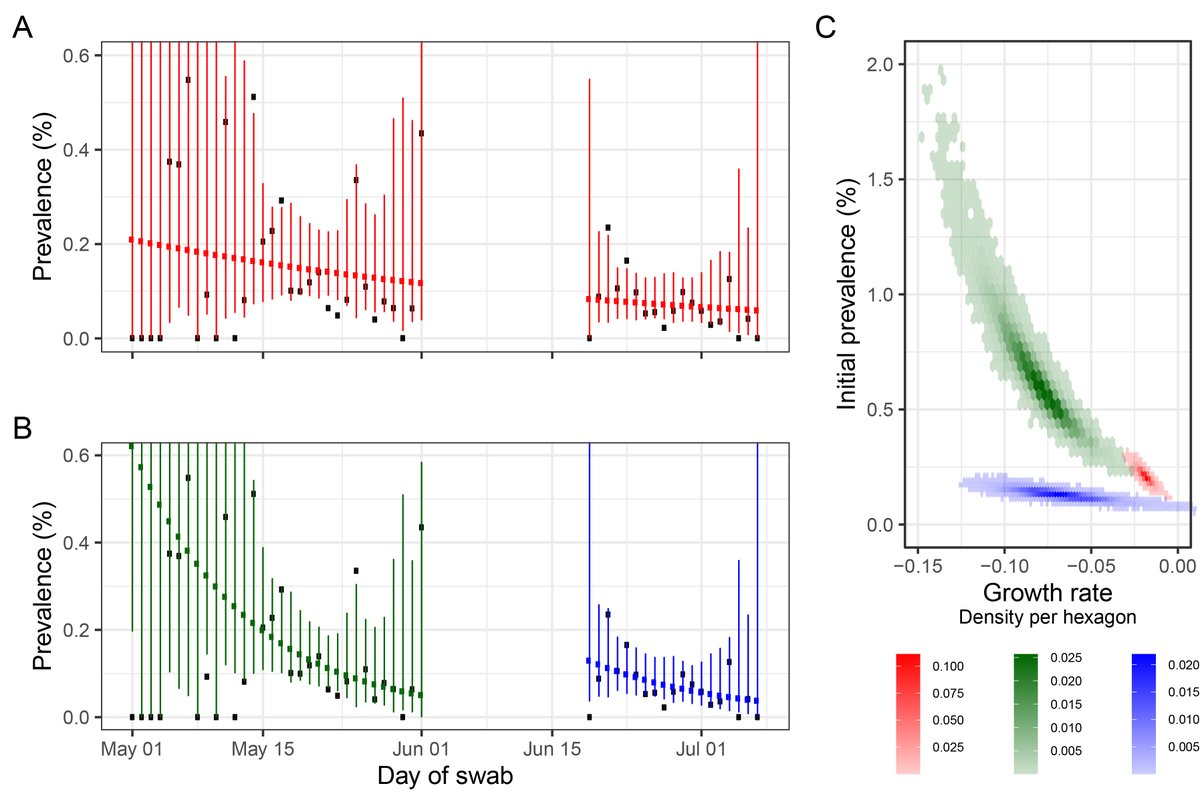
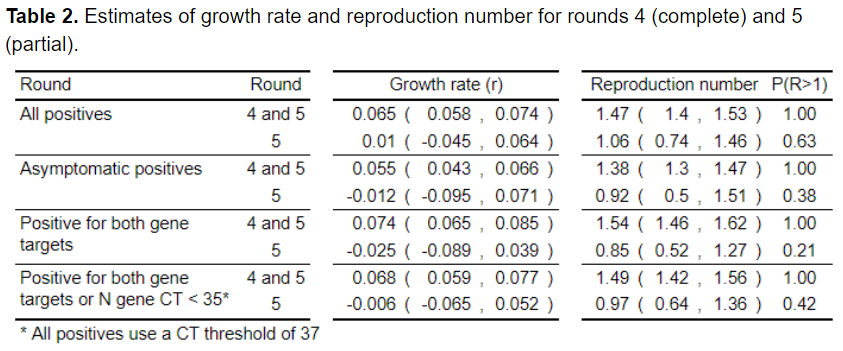
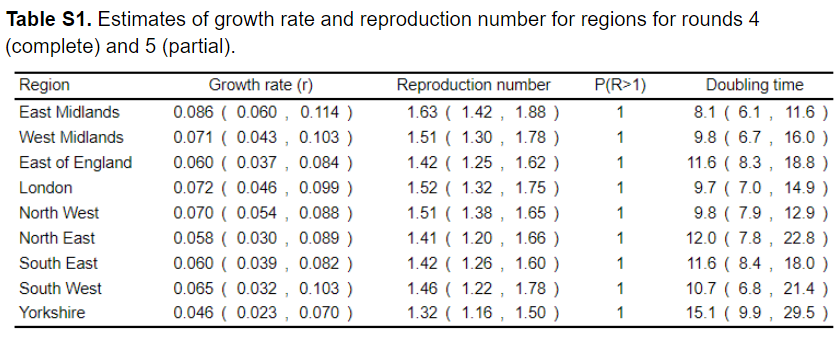
- We estimate doubling time of 10.6 (9.4, 12.0) days from 20 Aug to 26 Sep
- This corresponds to a R of 1.47 (1.40, 1.53)
- Using data only from round 5 (18 Sep to 26 Sep) we estimate a R of 1.06 (0.74, 1.46) with probability of 63% that R is greater than 1.
- This corresponds to a R of 1.47 (1.40, 1.53)
- Using data only from round 5 (18 Sep to 26 Sep) we estimate a R of 1.06 (0.74, 1.46) with probability of 63% that R is greater than 1.
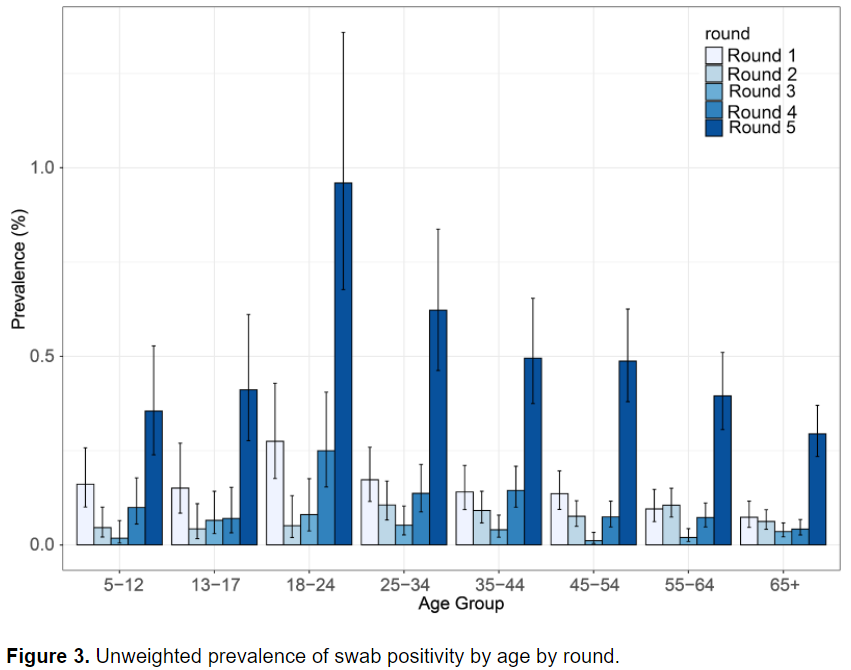
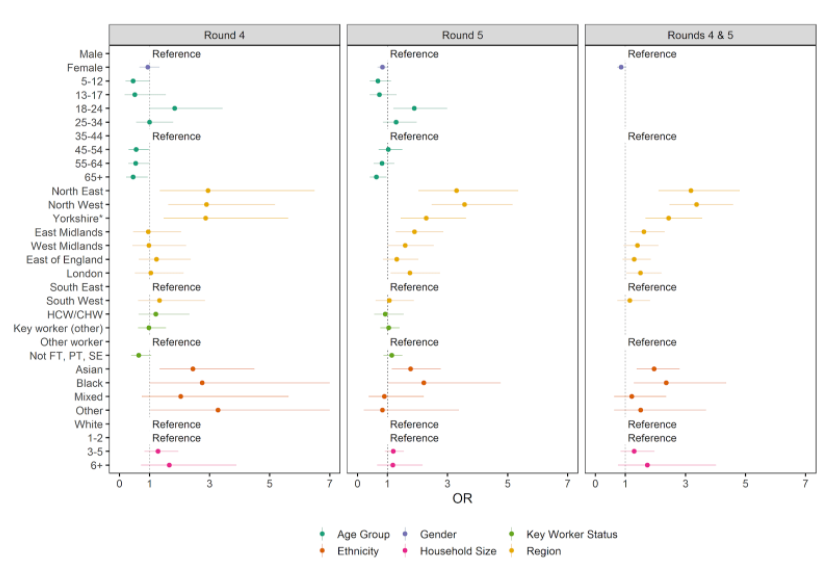
- Between rounds 4&5 there was a marked increase in unweighted prevalence at all ages.
- In most recent data, prevalence was highest in 18-24 yrs age group at 0.96% (0.68%, 1.36%)
- 65+ yrs prev increased ~7-fold b/w rounds 4&5 from 0.04% (0.03%, 0.07%) to 0.29% (0.23%, 0.37%)
- In most recent data, prevalence was highest in 18-24 yrs age group at 0.96% (0.68%, 1.36%)
- 65+ yrs prev increased ~7-fold b/w rounds 4&5 from 0.04% (0.03%, 0.07%) to 0.29% (0.23%, 0.37%)
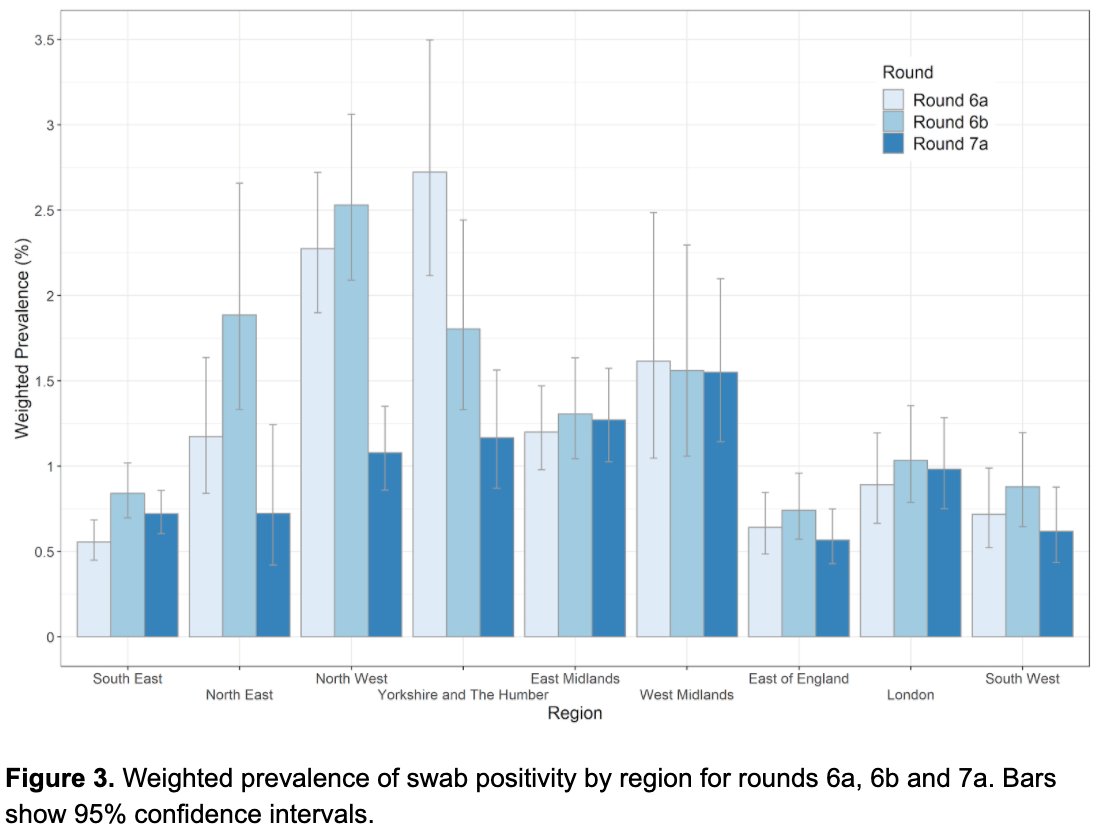
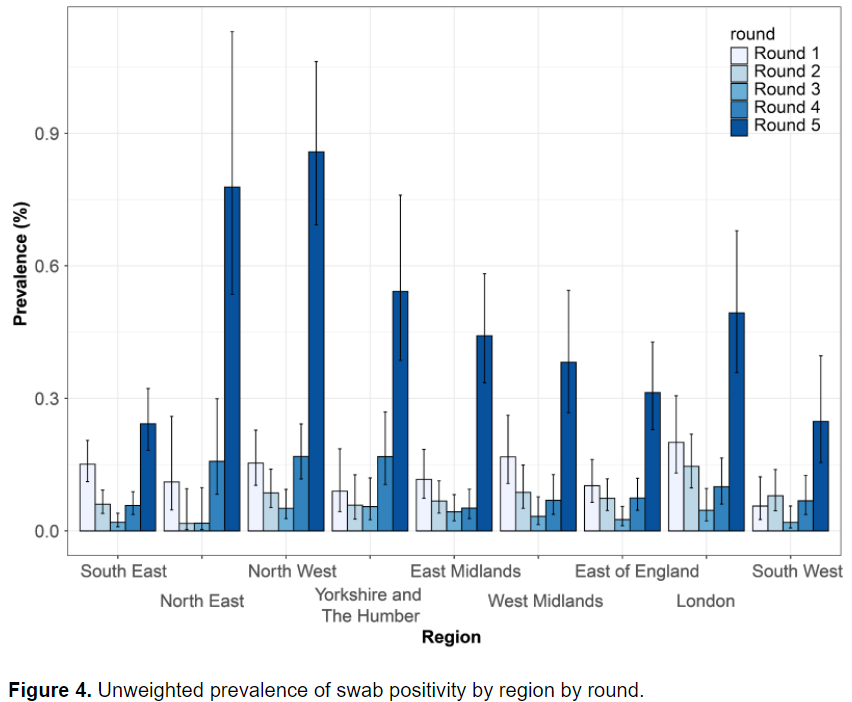
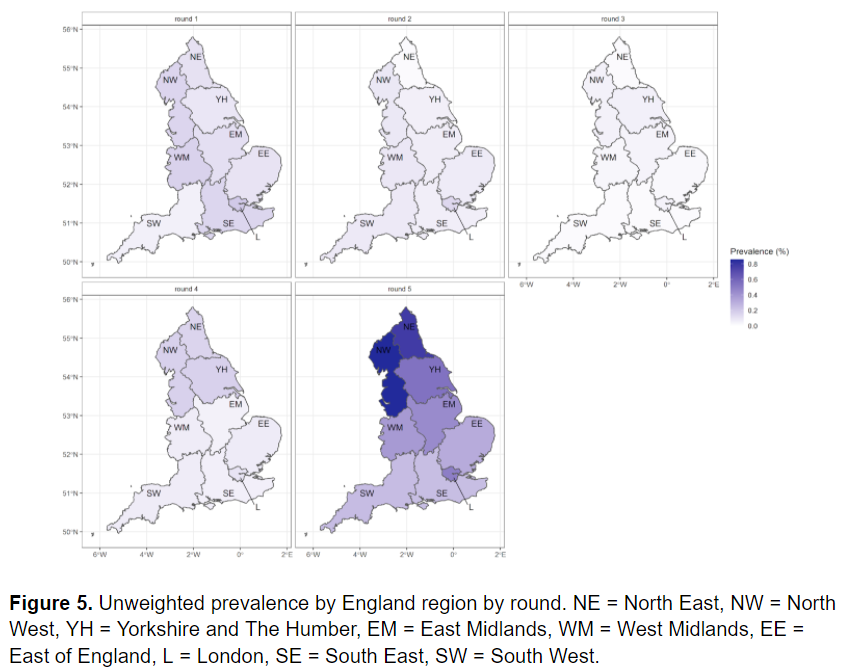
- Prev increased in all regions b/w rounds 4&5
- Highest unweighted prev in r5 was in the North West at 0.86% (0.69%, 1.06%)
- London prev increased ~5-fold: 0.10% (0.06%, 0.17%) to 0.49% (0.36%, 0.68%)
- R ranged from 1.32 (1.16,1.50), Yorkshire to 1.63 (1.42, 1.88), E Midlands
- Highest unweighted prev in r5 was in the North West at 0.86% (0.69%, 1.06%)
- London prev increased ~5-fold: 0.10% (0.06%, 0.17%) to 0.49% (0.36%, 0.68%)
- R ranged from 1.32 (1.16,1.50), Yorkshire to 1.63 (1.42, 1.88), E Midlands
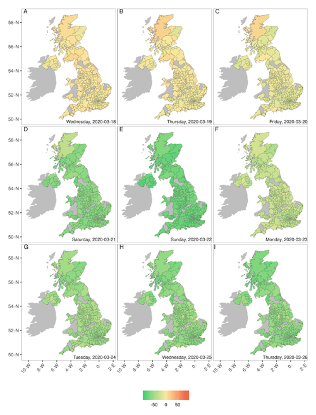
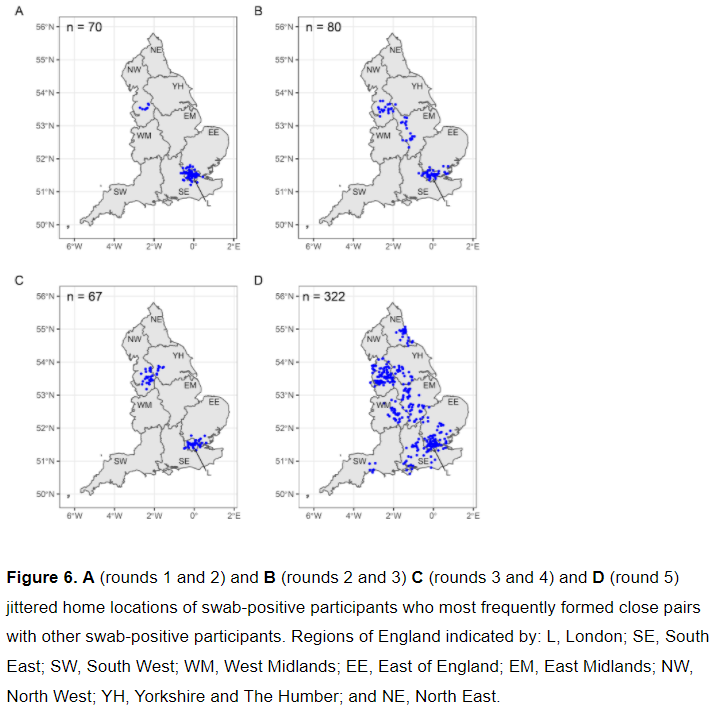
- There was extensive clustering in North West, Midlands, and London w/ pockets of clustering in other regions including South West, North East, and East of England.
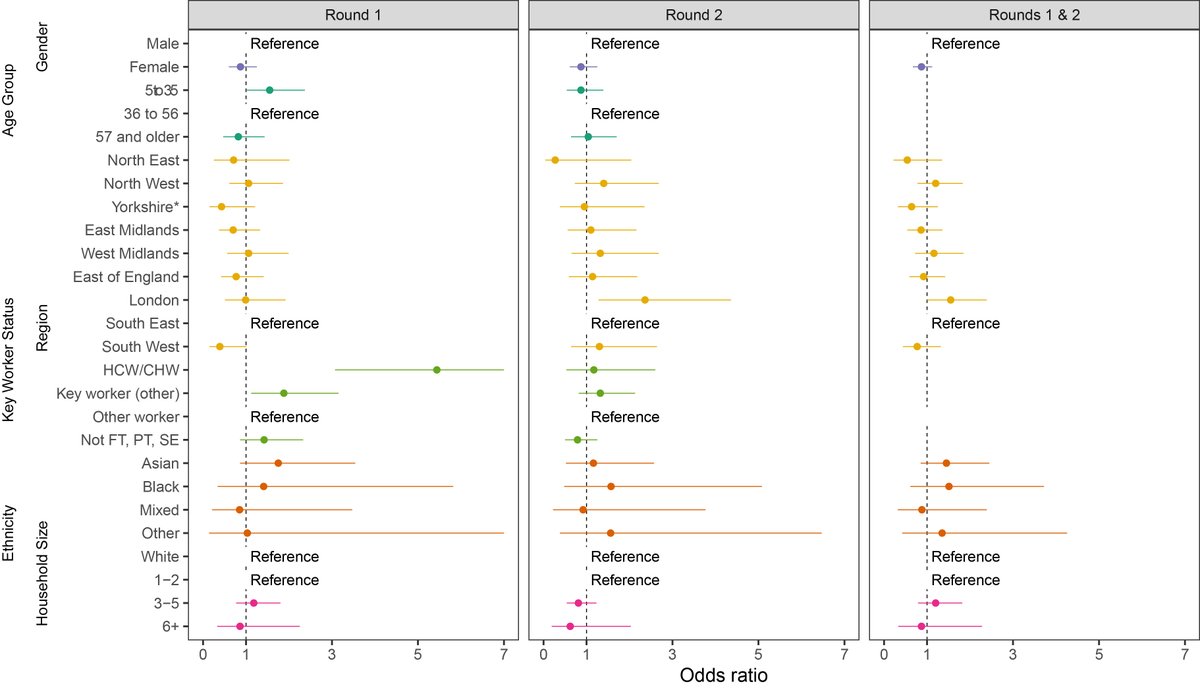
- Odds of infection were ~2-fold higher in people of Asian and Black ethnicity compared to white participants .
- Odds of infection were ~2-fold higher in people of Asian and Black ethnicity compared to white participants .
Conclusions:
- Since mid-August when we first detected a rise in prevalence, there has been a resurgence of the virus in the community
- Rates are higher now than at any time since we started measuring prevalence in May 2020.
- Since mid-August when we first detected a rise in prevalence, there has been a resurgence of the virus in the community
- Rates are higher now than at any time since we started measuring prevalence in May 2020.
- There is an urgent need for increasing public health efforts to reduce transmission of the virus in the community
- The primary aim should be to limit hospitalisations and deaths from COVID-19 that will inevitably follow the current high prevalence of SARS-CoV-2 infection
- The primary aim should be to limit hospitalisations and deaths from COVID-19 that will inevitably follow the current high prevalence of SARS-CoV-2 infection
Limitations:
- Possible differential responses to taking part in the study
- Some of the recent rise in prev may be explained by difficulties in obtaining a PCR test through routine testing programme
- A nose and throat swab may have limited sensitivity (~70%) to detect virus
- Possible differential responses to taking part in the study
- Some of the recent rise in prev may be explained by difficulties in obtaining a PCR test through routine testing programme
- A nose and throat swab may have limited sensitivity (~70%) to detect virus
This is an interim report as we are still getting data from round 5. A pre-print on the complete round 5 results will follow. Stay tuned.
As always, thank you to all of the participants for taking part and for all of our collaborators.
@SRileyIDD @DrCWalters @KellyIpsosMORI
As always, thank you to all of the participants for taking part and for all of our collaborators.
@SRileyIDD @DrCWalters @KellyIpsosMORI
• • •
Missing some Tweet in this thread? You can try to
force a refresh