1/G
Interesting method from @GidMK and co-authors for calculating IFR from PCR-based cases.
(IFR is the proportion of SARS-CoV-2-infected people who die COVID-19;
PCR measures viral genetic material in people;
Cases are people who were infected)
medrxiv.org/content/medrxi…
Interesting method from @GidMK and co-authors for calculating IFR from PCR-based cases.
(IFR is the proportion of SARS-CoV-2-infected people who die COVID-19;
PCR measures viral genetic material in people;
Cases are people who were infected)
medrxiv.org/content/medrxi…

2/G
The basic idea is that some countries had relatively few infected, and tested with PCR so thoroughly, that their PCR testing got a relatively large proportion of infected people.
Iceland is used a baseline example:
medrxiv.org/content/medrxi…
The basic idea is that some countries had relatively few infected, and tested with PCR so thoroughly, that their PCR testing got a relatively large proportion of infected people.
Iceland is used a baseline example:
medrxiv.org/content/medrxi…

3/G
Their method yields a range of IFR values consistent with those from serology [i.e. antibody testing], which provides independent validation for their method.
green: their PCR-based methods
blue: Serology-based estimates
medrxiv.org/content/10.110…
Their method yields a range of IFR values consistent with those from serology [i.e. antibody testing], which provides independent validation for their method.
green: their PCR-based methods
blue: Serology-based estimates
medrxiv.org/content/10.110…

4/G
This includes confirmation by research published after their method. For example:
Their Iceland IFR: ~0.4%
Ice serology study: 0.3% (CI: 0.2% - 0.6%)
nejm.org/doi/full/10.10…
This includes confirmation by research published after their method. For example:
Their Iceland IFR: ~0.4%
Ice serology study: 0.3% (CI: 0.2% - 0.6%)
nejm.org/doi/full/10.10…
5/G
Another example:
Their South Korea IFR: ~0.8%
Serology study: ~0.8%
(assuming the 1 positive result out of 1440 is not a false positive; ~36,000 infections, ~300 deaths 4 weeks after study mid-point)
ourworldindata.org/coronavirus-da…
cdc.go.kr/board/board.es…
Another example:
Their South Korea IFR: ~0.8%
Serology study: ~0.8%
(assuming the 1 positive result out of 1440 is not a false positive; ~36,000 infections, ~300 deaths 4 weeks after study mid-point)
ourworldindata.org/coronavirus-da…
cdc.go.kr/board/board.es…

6/G
There are other PCR-based methods for estimating IFR. Below is an example for Stockholm, Sweden (@GidMK's method wouldn't work there, since they didn't catch a large enough proportion of their cases).
web.archive.org/web/2020092621…
There are other PCR-based methods for estimating IFR. Below is an example for Stockholm, Sweden (@GidMK's method wouldn't work there, since they didn't catch a large enough proportion of their cases).
web.archive.org/web/2020092621…

7/G
That PCR-based IFR fits with modelling from other data.
There are also seroprevalence results, tho the method from @GidMK's method wouldn't apply, since Stockholm's pandemic was not then well-contained
kth.se/en/aktuellt/ny…
sll.se/verksamhet/hal…
medrxiv.org/content/10.110…
That PCR-based IFR fits with modelling from other data.
There are also seroprevalence results, tho the method from @GidMK's method wouldn't apply, since Stockholm's pandemic was not then well-contained
kth.se/en/aktuellt/ny…
sll.se/verksamhet/hal…
medrxiv.org/content/10.110…

8/G
Next step might be to compare the results of @GidMK's method to serology-based IFRs for Australia, New Zealand, + Lithuania.
A recent Australian study won't be help, since its population is very non-representative of the general population.
Next step might be to compare the results of @GidMK's method to serology-based IFRs for Australia, New Zealand, + Lithuania.
A recent Australian study won't be help, since its population is very non-representative of the general population.
https://twitter.com/GidMK/status/1306840004656685056
9/G
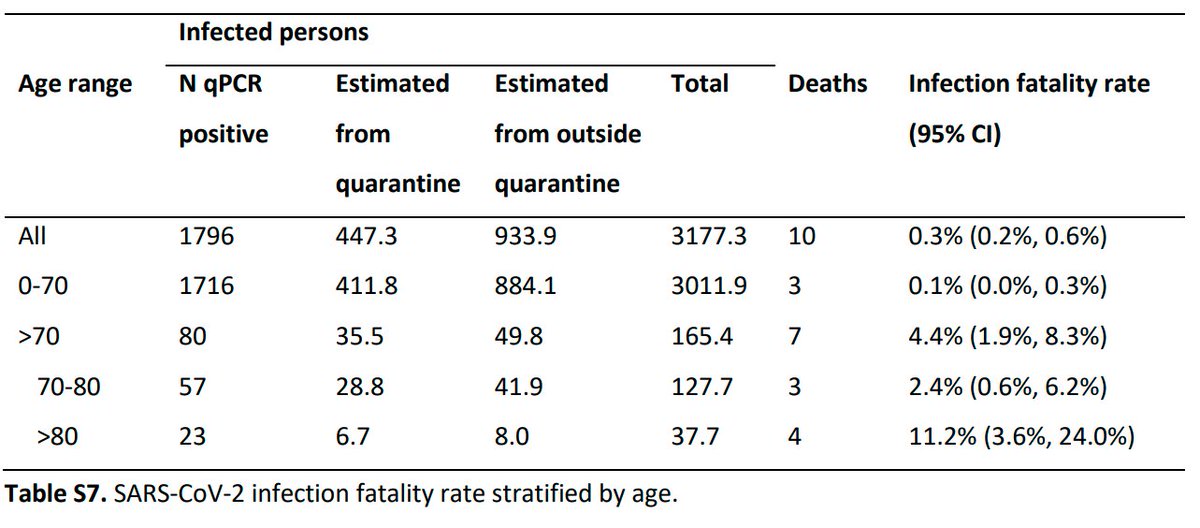
Their serology-based method and PCR-based methods also fits with PCR-based IFR results from the Diamond Princess (a cruise ship on which many people were infected with SARS-CoV-2, with 14 dying of COVID-19).
page 32:
medrxiv.org/content/medrxi…
Their serology-based method and PCR-based methods also fits with PCR-based IFR results from the Diamond Princess (a cruise ship on which many people were infected with SARS-CoV-2, with 14 dying of COVID-19).
https://twitter.com/AtomsksSanakan/status/1283302606065020928
page 32:
medrxiv.org/content/medrxi…

• • •
Missing some Tweet in this thread? You can try to
force a refresh