
💥New meta-analysis reports CV, Kidney & Mortality outcomes with SGLT2i use with & without Metformin
👉🏽
⚡️Before reviewing the meta-analysis check out this Tweetorial on Should Metformin be the 1st line therapy in T2DM patients?👇🏽
1/ dom-pubs.onlinelibrary.wiley.com/doi/10.1111/do…

👉🏽
⚡️Before reviewing the meta-analysis check out this Tweetorial on Should Metformin be the 1st line therapy in T2DM patients?👇🏽
1/ dom-pubs.onlinelibrary.wiley.com/doi/10.1111/do…
https://twitter.com/aishaikh/status/1167550464726044672

⚡️In the meta-analysis, 6 SGLT2i vs Placebo RCTs were included:
-4 trials were CV outcome trials (EMPA-REG, CANVAS, DECLARE-TIMI, VERTIS-CV)
-1 trial was a Kidney outcome trial
(CREDENCE)
-1 trial was a Heart Failure trial
(DAPA-HF)
2/
-4 trials were CV outcome trials (EMPA-REG, CANVAS, DECLARE-TIMI, VERTIS-CV)
-1 trial was a Kidney outcome trial
(CREDENCE)
-1 trial was a Heart Failure trial
(DAPA-HF)
2/


💥Total number of participants from the 6 RCTs were 51,743
💥Baseline Metformin use varied across the trials as shown below:
⚡️21% in DAPA-HF
⚡️58% in CREDENCE
⚡️74%-82% in EMPA-REG, CANVAS,
DECLARE-TIMI, VERTIS-CV
3/
💥Baseline Metformin use varied across the trials as shown below:
⚡️21% in DAPA-HF
⚡️58% in CREDENCE
⚡️74%-82% in EMPA-REG, CANVAS,
DECLARE-TIMI, VERTIS-CV
3/
💥Results: CV outcome
⚡️SGLT2i ⬇️ major adverse cardiovascular events regardless of baseline Metformin use 👇🏽
⚡️SGLT2i ⬇️ hospitalization for heart failure & CV death👇🏽
4/
⚡️SGLT2i ⬇️ major adverse cardiovascular events regardless of baseline Metformin use 👇🏽
⚡️SGLT2i ⬇️ hospitalization for heart failure & CV death👇🏽
4/

💥Results:Kidney outcome & All-cause mortality
⚡️SGLT2i ⬇️ worsening of kidney function, ESKD, kidney death similarly in pts. receiving Metformin vs patients not receiving Metformin
⚡️SGLT2i ⬇️ risk of all-cause mortality regardless of Metformin use 👇🏽
5/
⚡️SGLT2i ⬇️ worsening of kidney function, ESKD, kidney death similarly in pts. receiving Metformin vs patients not receiving Metformin
⚡️SGLT2i ⬇️ risk of all-cause mortality regardless of Metformin use 👇🏽
5/

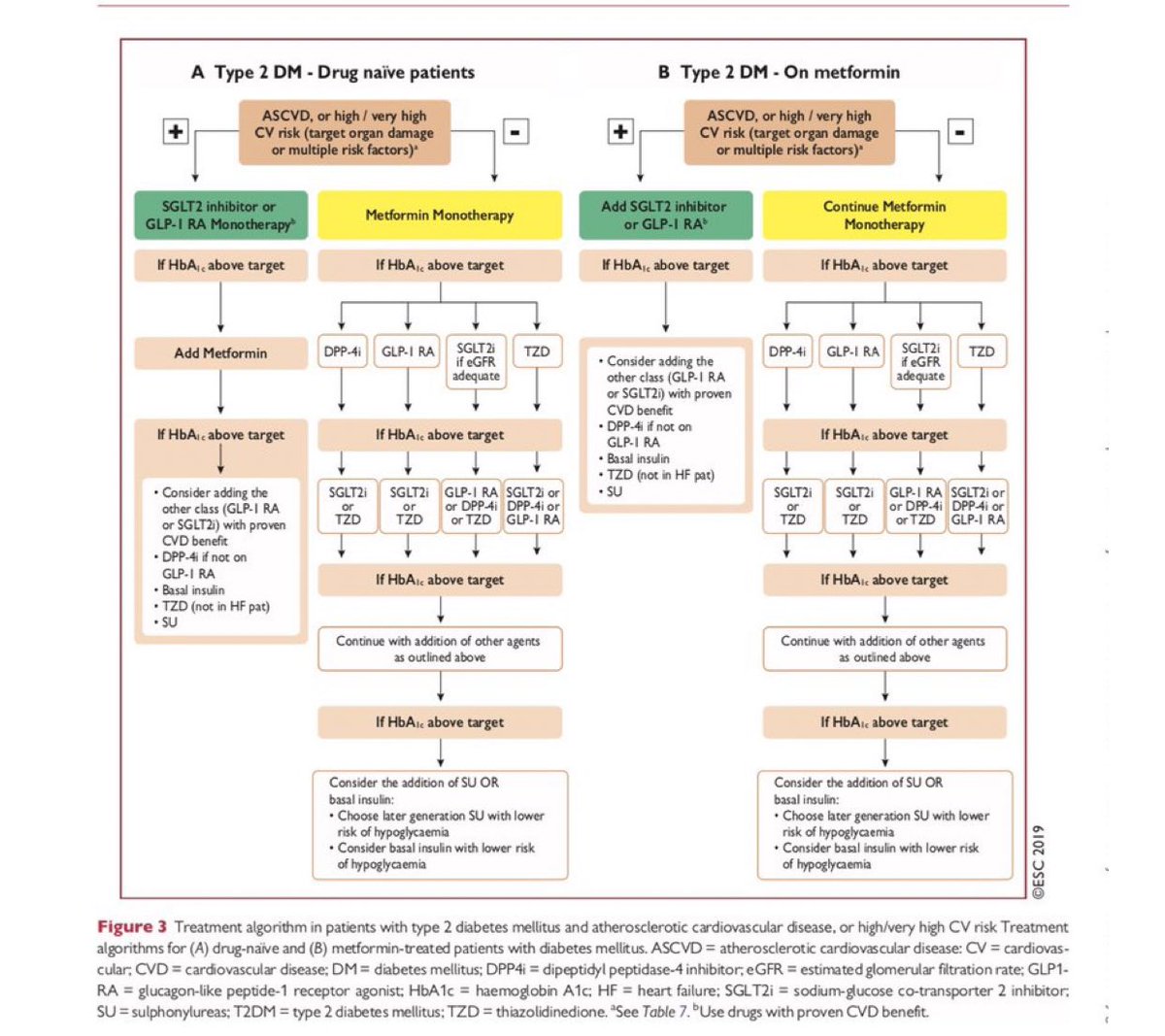
💥So should Metformin be the 1st-line therapy for T2DM patients especially the patients at high risk for CV events?
⚡️The European Society of Cardiology changed their recommendations last year - see below👇🏽
⚡️Should other societies follow?
End/
⚡️The European Society of Cardiology changed their recommendations last year - see below👇🏽
⚡️Should other societies follow?
End/
• • •
Missing some Tweet in this thread? You can try to
force a refresh
















