A thread on where we are with the COVID-19 pandemic in England, and what we need to do urgently based on current evidence. This thread also explores why the govt Tier 1-3 strategy is nothing but a distraction from the actual public health response needed. 1/N
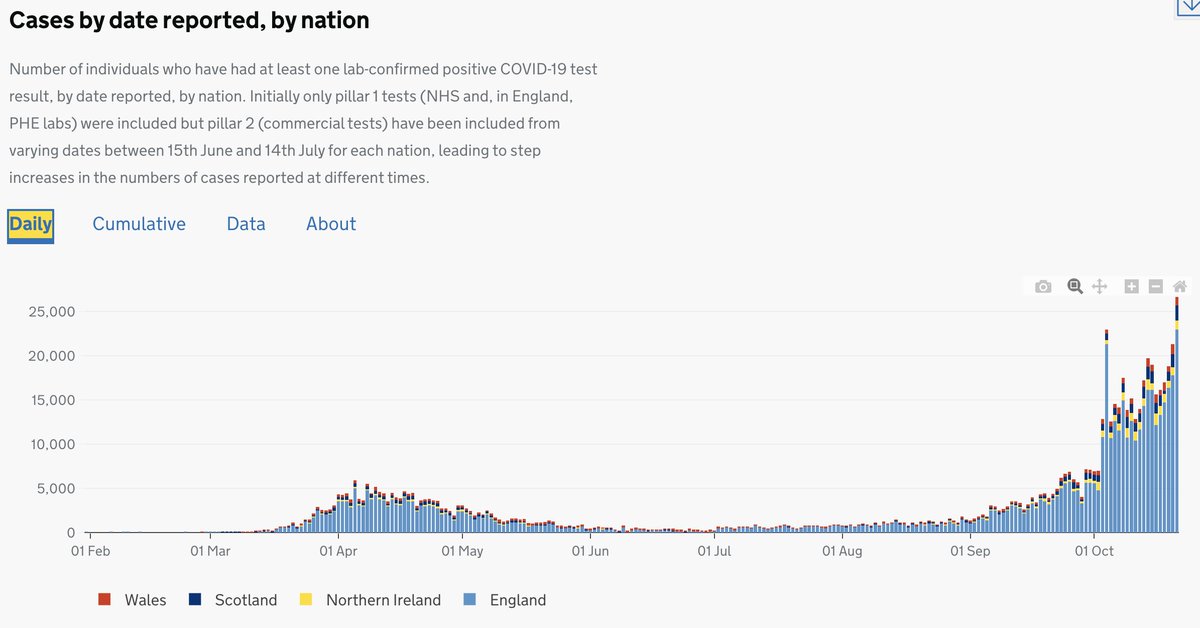
As we know, the PHE data shows an exponential increase in daily confirmed cases of COVID-19. We are currently seeing between 25-30K daily cases. This is likely an underestimate as testing capacity has been reached. Moreover, increases are occurring across all of England. 2/N 
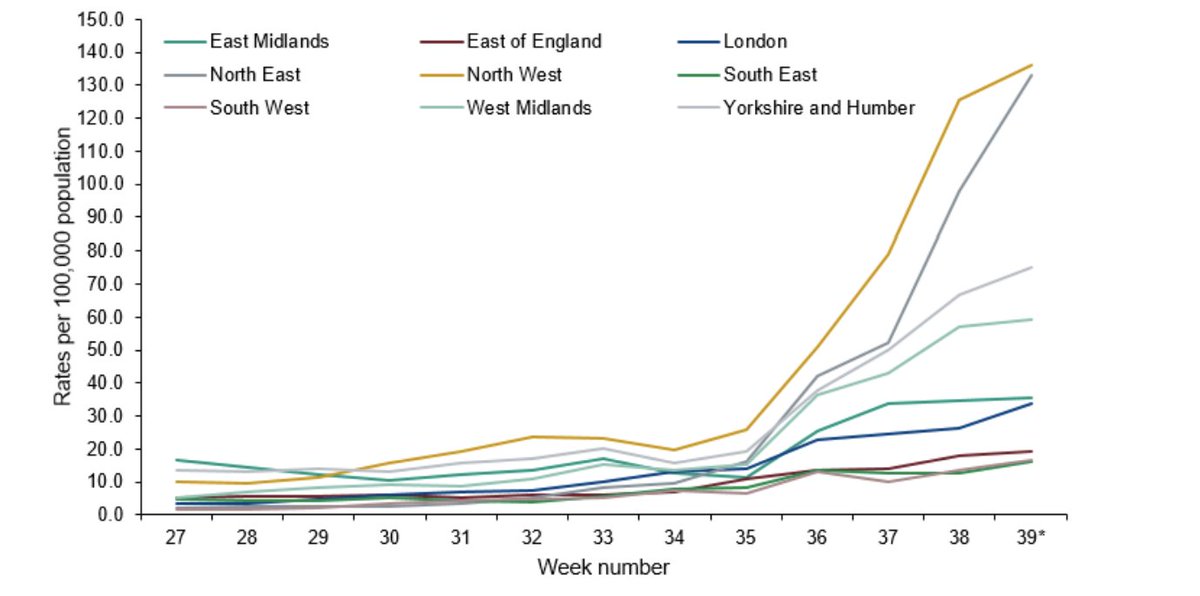
Predictably increase in case numbers have translated over time into increasing hospitalisations across all of England, with regions in the North likely to hit NHS capacity soon if we don't act. While increases in the South appear slower, these are only lagging 3-4 wks behind. 3/N
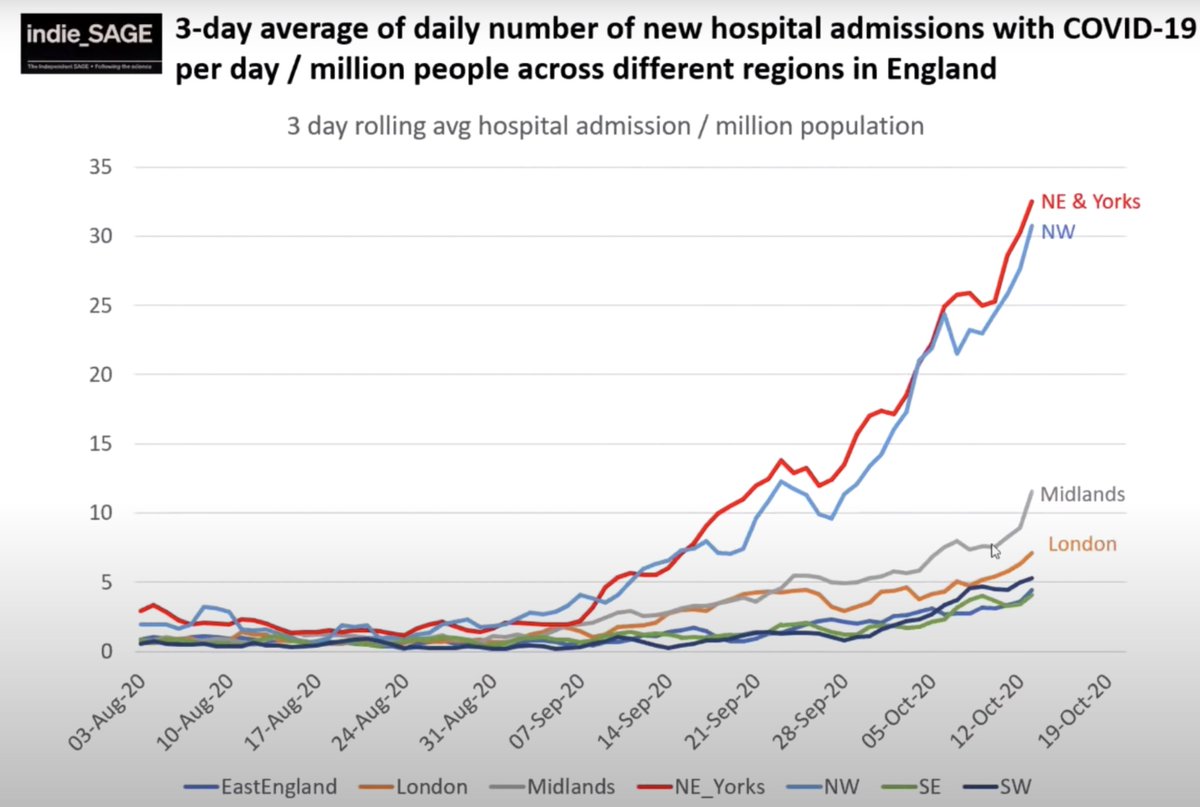
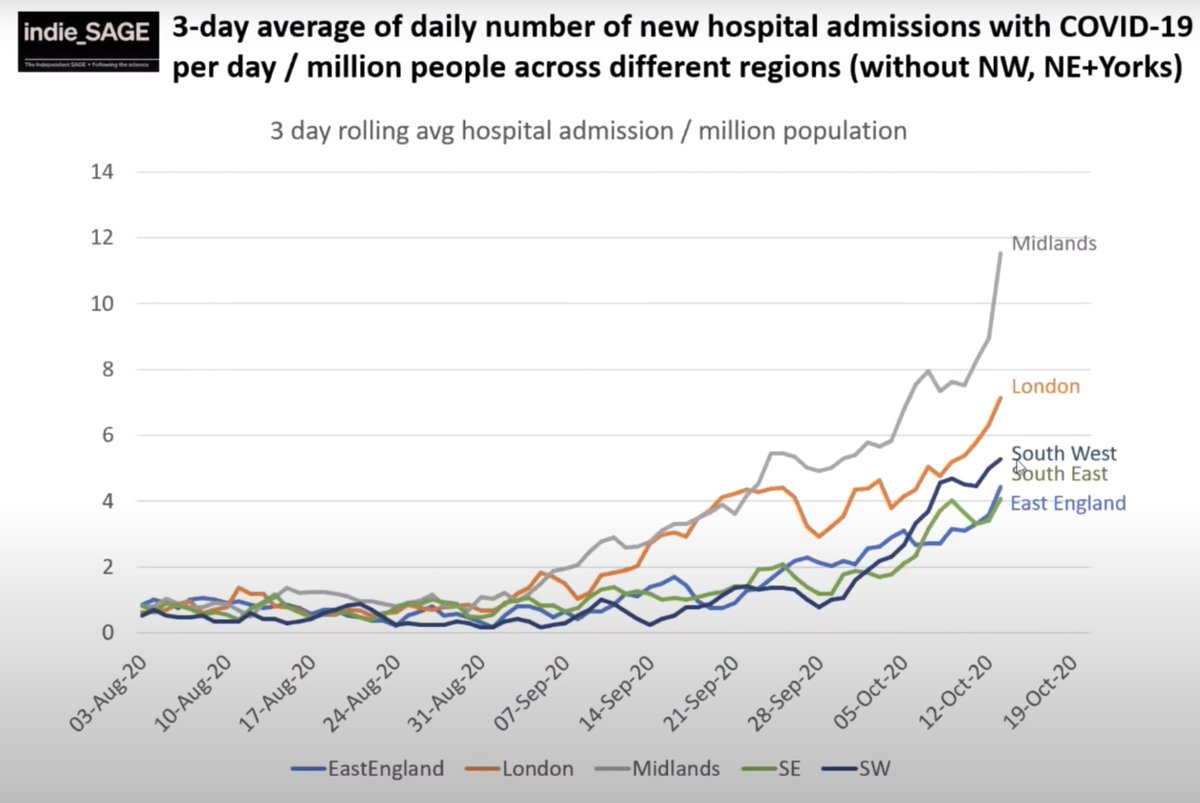
We know that hospitalisations are doubling every 14 days in England (@IndependentSage)- with clear exponential rises. This is likely to translate into corresponding increases in deaths with a 2-3 wk time lag from increase in hospitalisations. 4/N
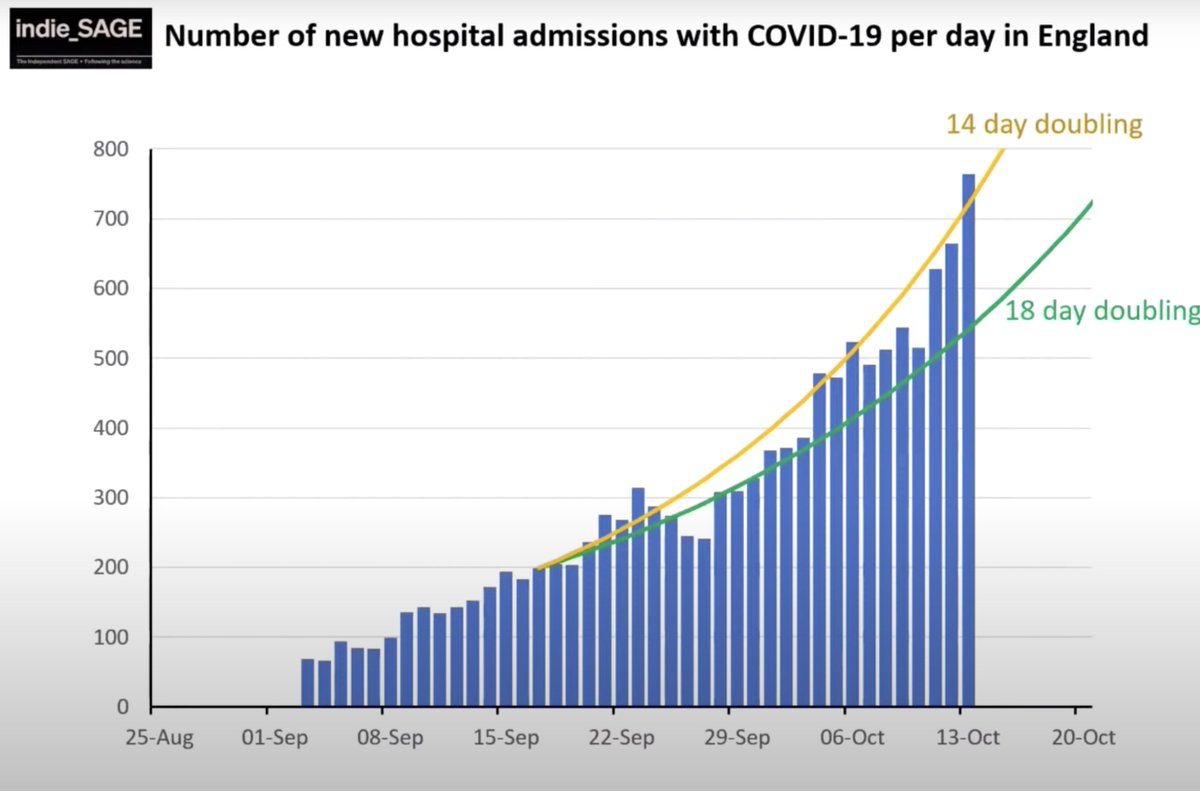
As there is a lag of ~4 wks from infection to death, even if we act now, we will sadly see increasing deaths over at least the next 4 wk period. We are likely to see ~2000 deaths in the next 2 wks, ~4000 in the 2 wks after, and ~8000 in the 2 wks after. 5/N
This means that many of those who will die from now to November have already been infected, and there is little we can do to prevent this. We can only manage these cases the best possible way in hospital. The most effective way to prevent deaths is to prevent infections. 6/N
This means we will inevitably now see ~6-10K deaths by December due to late action. But we can prevent more if we act quickly! What do we need to do to prevent these deaths, and more people being sick with Long COVID-19. 7/N
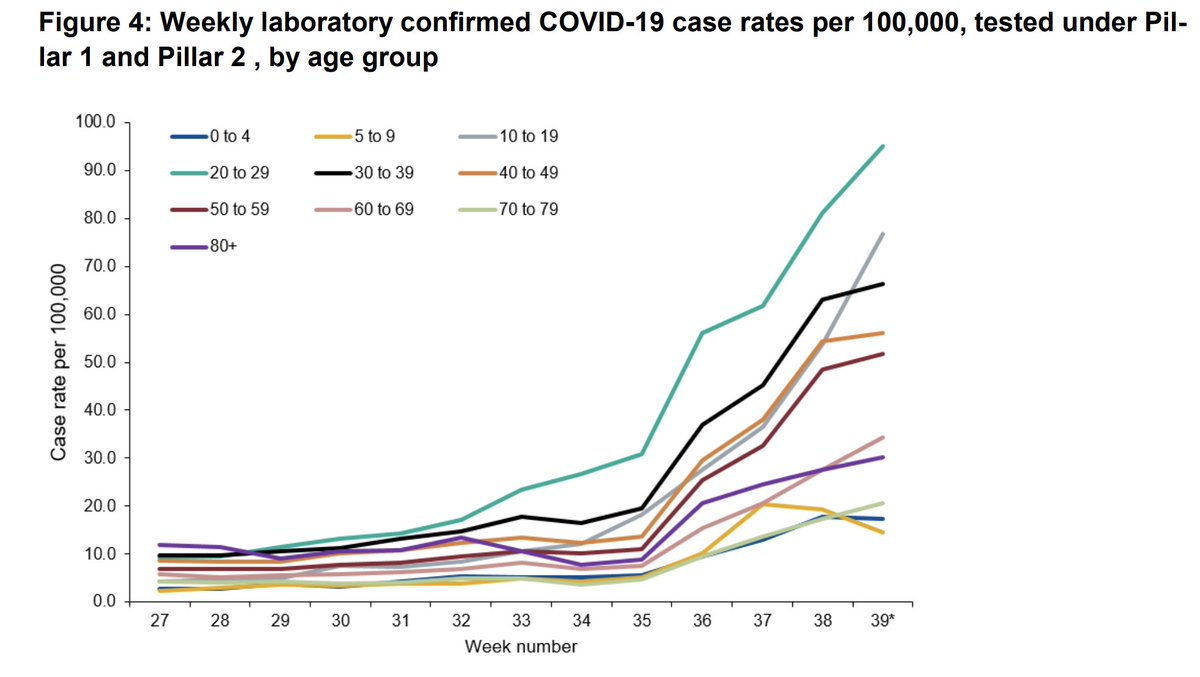
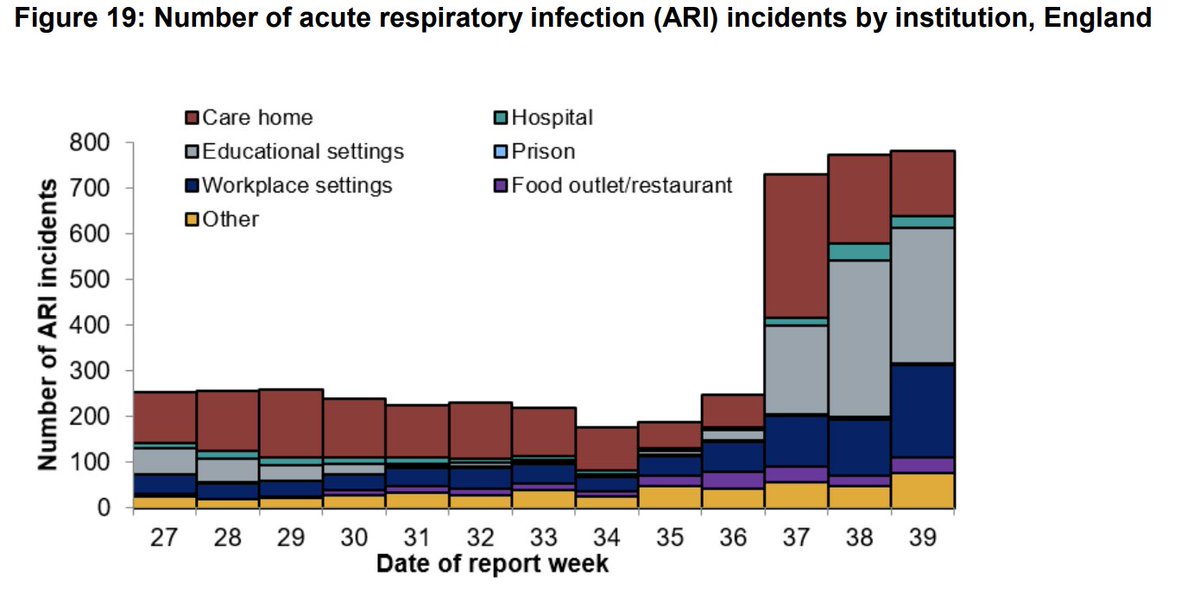
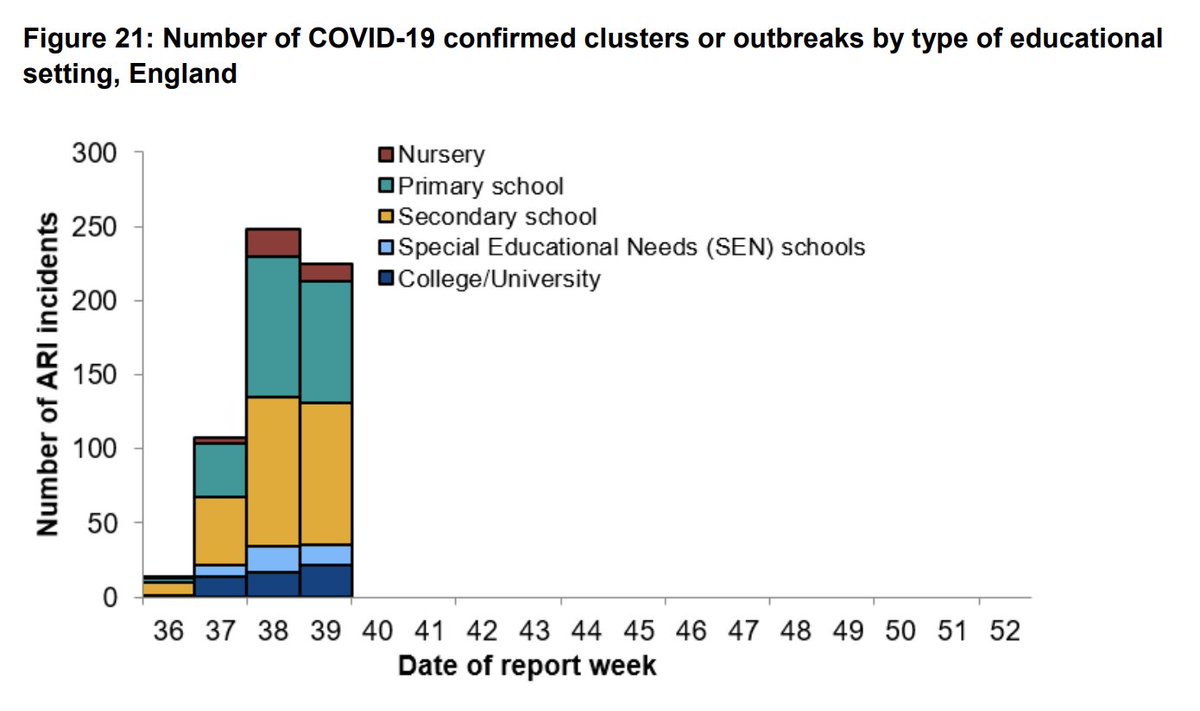
Cases are rising across all age groups, and across many different settings. Educational settings, including primary and secondary schools are important hubs of transmission. Using a piecemeal approach targeting only hospitality and households, as Tier1-3 do will not work. 8/N
Experts, including SAGE, iSAGE, and the CMO all agree that we need a multi-pronged approach, rather than the Tier1-3 approach. There has been little to no impact of restrictions imposed in such a piecemeal manner. 9/N
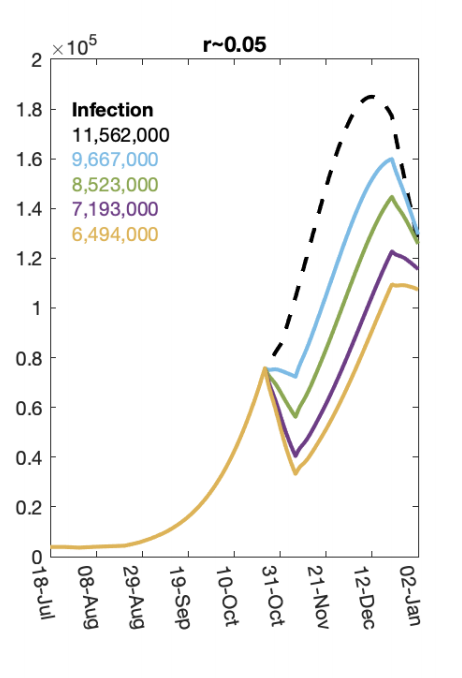
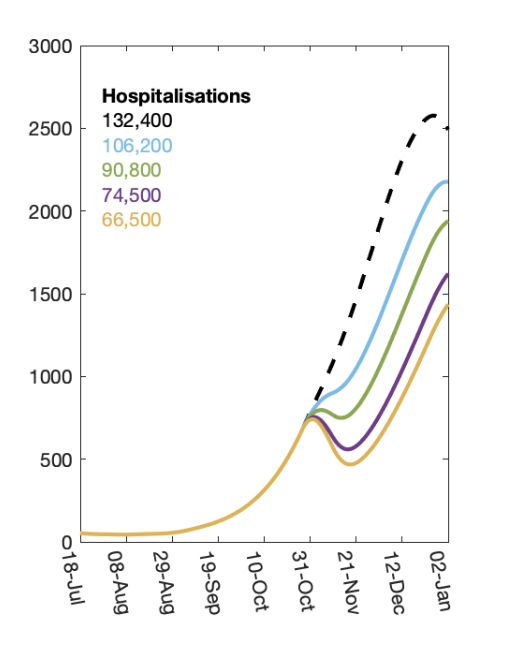
There is agreement that we need an urgent circuit breaker to curb transmission. SAGE modelling shows that a 2 wk circuit breaker could have a huge impact on case numbers, hospitalisations and deaths if introduced now. The more effectively we reduce R, the more lives we save. 10/N

But what does this mean for long-term strategy?
The idea of the March lockdown was to rapidly bring down cases, and buy time to develop good case finding systems (TTI) to enable us to then control local outbreaks effectively without needing nation-wide restrictions. 11/N
The idea of the March lockdown was to rapidly bring down cases, and buy time to develop good case finding systems (TTI) to enable us to then control local outbreaks effectively without needing nation-wide restrictions. 11/N
Despite having several months to prepare, we failed to develop an effective system. The slide here shows the stark contrast between the private (Serco) system, and the NHS test, trace system. If we invest in NHS based TTI, we can have effective test, trace & isolate. 12/N
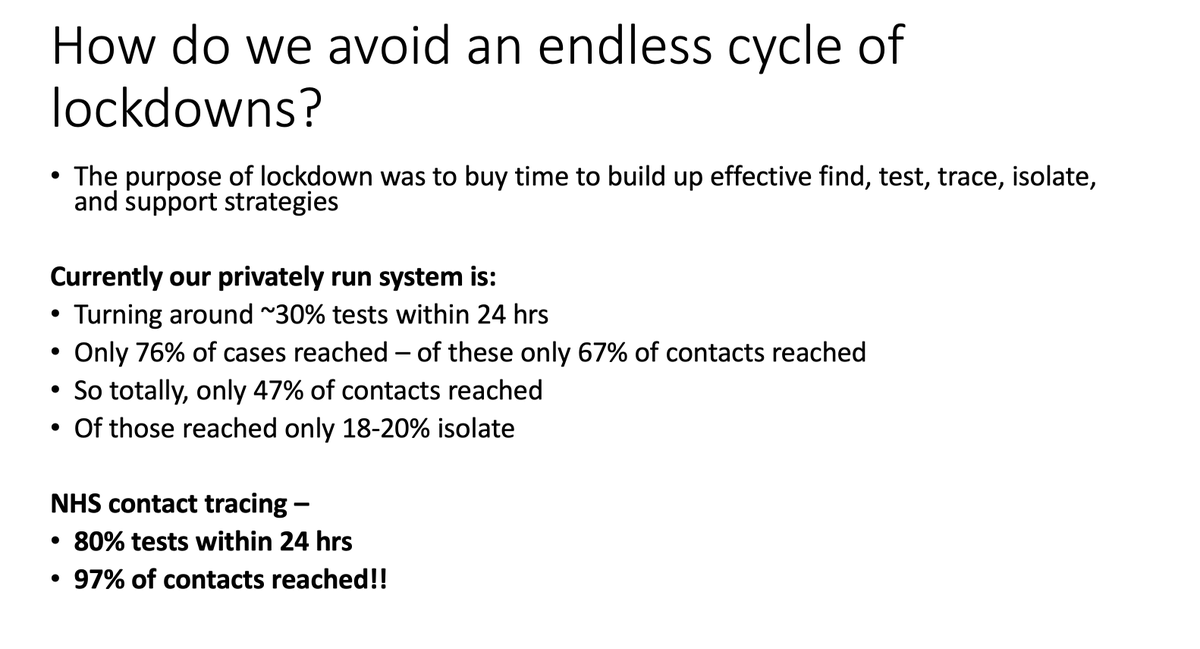
It's important that such a system is backed by financial support for those who need to isolate/work from home/shield. Scaling up testing is not going to solve the problem if only 18-20% of those who need to isolate are able to (due to financial insecurity). 13/N
Important to note here, that the idea of some sort of a trade-off between COVID-19 control and the economy is a false one. The evidence overwhelmingly shows that countries that have invested in robust COVID-19 control have had less of an impact to their economies. 14/N
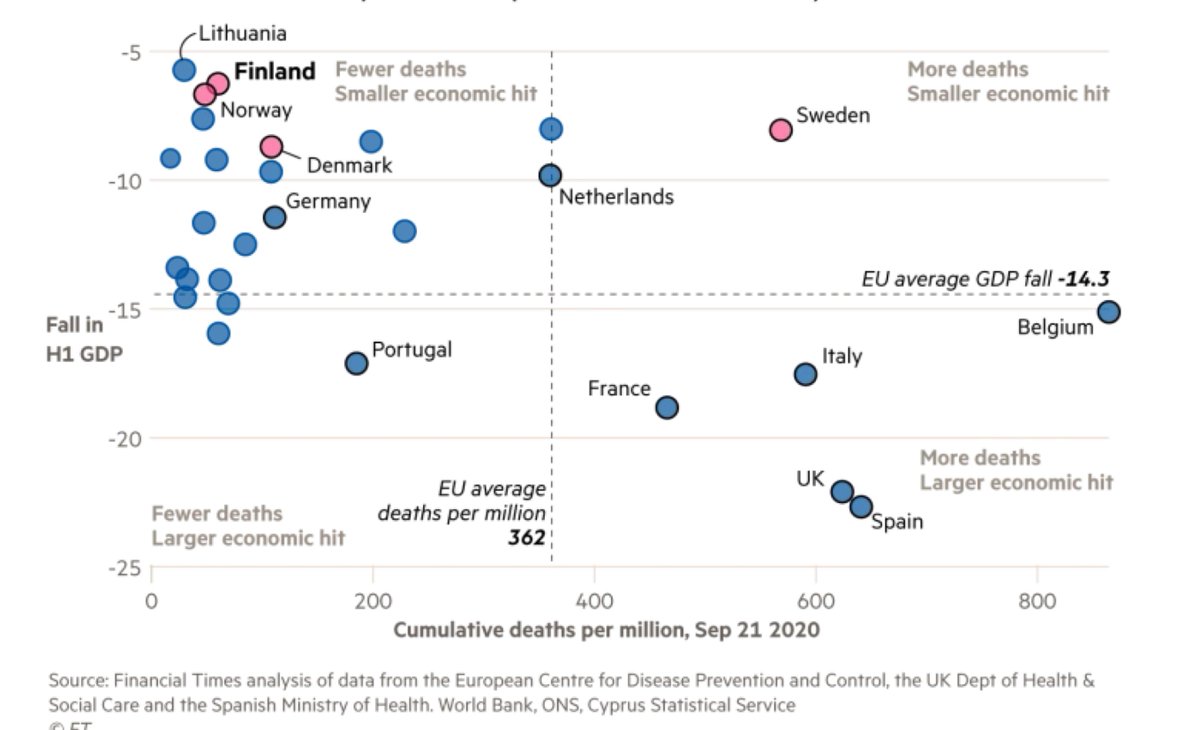
Similarly, the idea that COVID-19 control is divorced from providing routine healthcare to those with chronic conditions is also a false one. The more COVID-19 transmission is allowed to increase across the population, the more overwhelmed our health services will be. 15/N
The only way to protect the NHS, and enable it to provide routine care is to prevent COVID-19 infection, and prevent NHS services from being overwhelmed. Controlling COVID-19 is the only way to protect our health, and our economy. 16/N
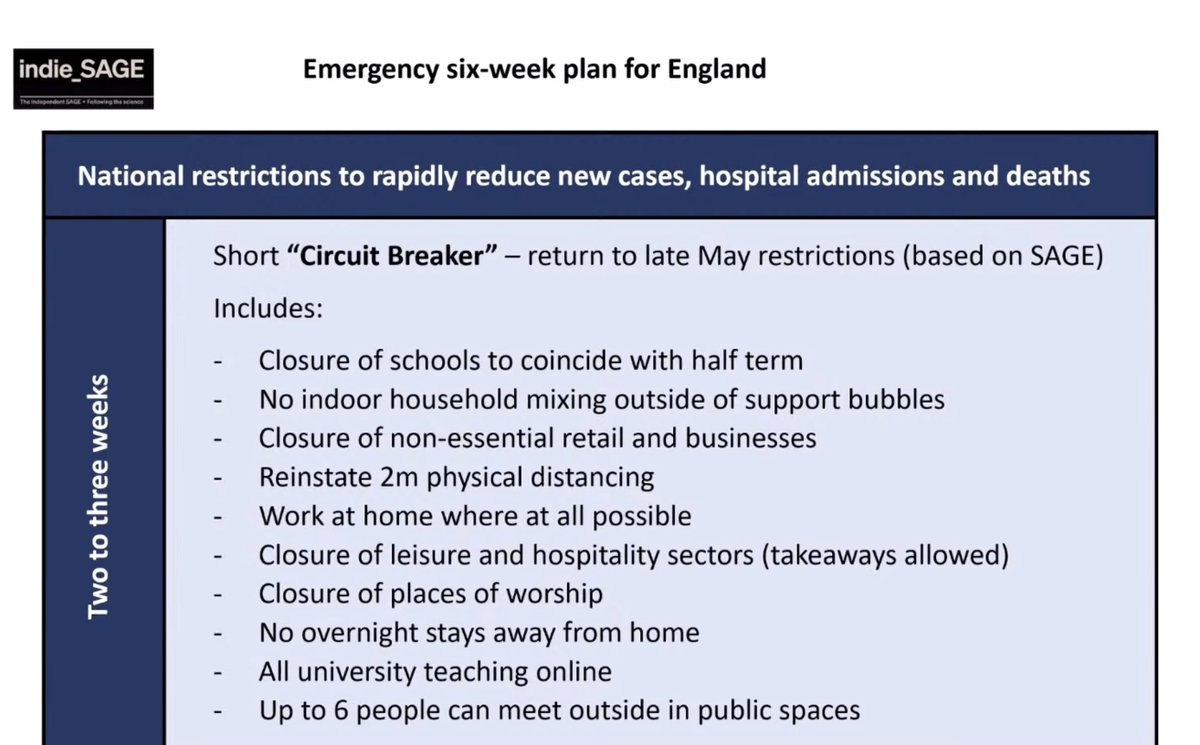
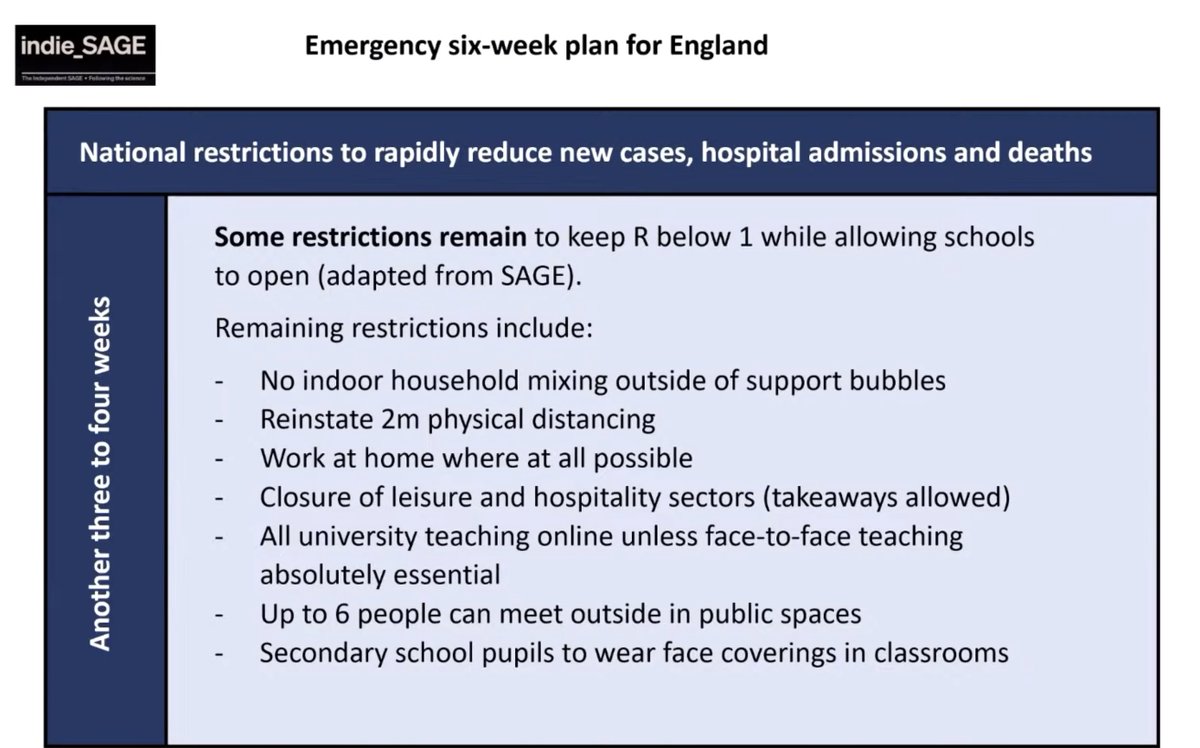
Here is the advice by @IndependentSage. They suggest a 2 wk circuit breaker (similar to May) followed by lower level restrictions over another 3-4 wks. This period needs to be used to urgently reform the current TTI system, and provide financial support to those affected. 17/N
It is crucial to utilise this period to put in place effective case detection strategies so we can rapidly identify and control outbreaks once nation-wide restrictions are lifted. Without this we will likely find ourselves in the same situation again. 18/N
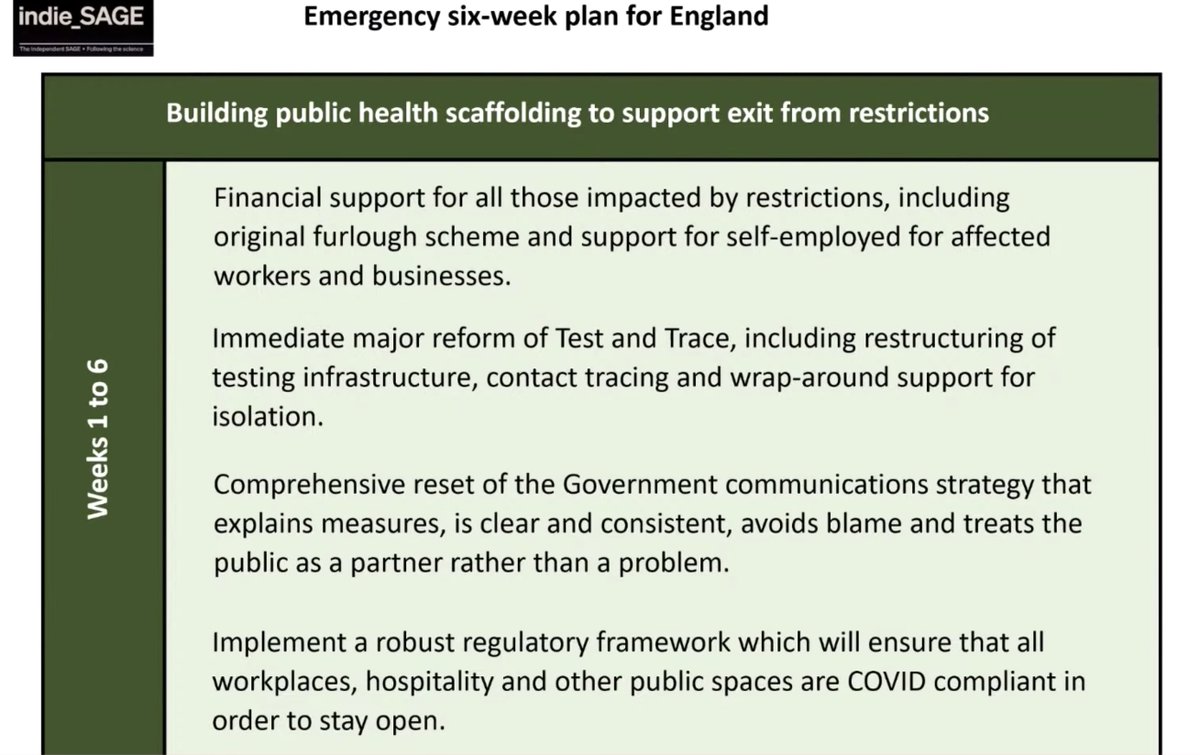
Financial support is a key part of this. We also need clear public health communication that doesn't minimise the risk posed by COVID-19 or blame the public. We also need clear regulatory frameworks for education, workplaces & other settings with support for these from govt. 19/N
We are very near seeing a repeat of March, and we're sleepwalking into a situation where tens of thousands of deaths will occur. We need to act now. Every day we wait results in hundreds of excess deaths. Inaction by govt is costing lives. 20/N
Importantly, we need a long term strategy so we are not stuck in an endless cycle of late action related lockdowns. We need effective and robust FTTIS systems so we are rapidly controlling outbreaks, as many other countries have done, without the need to return to lockdown. 21/N
We need to prevent the fire, rather than fight it once it's accelerated beyond control. END
• • •
Missing some Tweet in this thread? You can try to
force a refresh