Such a great experience working with this amazing group of co-authors examining the effect of NMBA in #ARDS ! ! In particular, @AlhazzaniW is one of the best mentors out there! This topic is of extremely high relevance with the COVID-19 pandemic. 1/ 

With the ROSE trial, there were legitimate questions raised re: utility of NMBA use in ARDS. ROSE, however, used a light sedation strategy which was different from the other studies. As expected, we found a subgroup difference in mortality when comparing according to sedation /2

As such, we could not pool the results of mortality all together as ROSE had a different population as part of their study /3
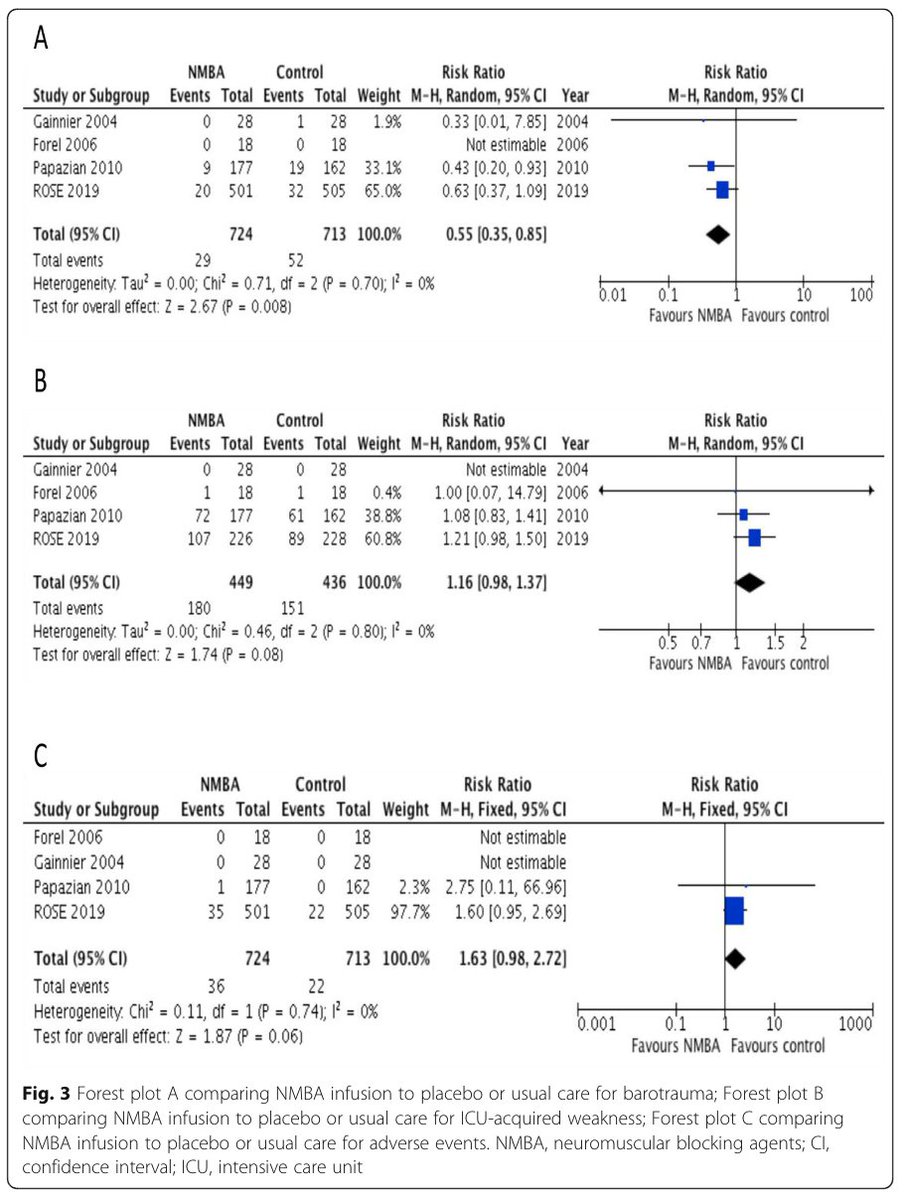
With respect to barotrauma, we found that NMBAs may be beneficial (RR 0.55; 95% CI 0.35-0.85). NMBAs effects on ICU acquired weakness and adverse events remains unclear /4
Bottom line: NMBAs had a mortality benefit in ARDS when compared to deep sedation but not when compared to light sedation /5
So how do we reconcile this: We have completed work on an upcoming ICM-RPG guideline that will be addressing this. Stay tuned! @yourICM 6/6
Once again, nice to see some great @MacEmerg and @MacCriticalCare collaboration. Also amazing to work with @ZDuhailib !! @MacDeptMed @MacCEprog
Full Article can be found here: icm-experimental.springeropen.com/articles/10.11…
@threadreaderapp Please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh