
1/24
#EPeeps, #EHRA_ESC is proud to have the new 2020 @escardio #AFib guidelines
Here’s my personal #tweetorial about the news and the highlights of these 126 pages.
I congratulate @GerdHindricks, @tanjapotpara1 & whole team for this tremendous work. #ESCGuidelines #EHRA_Ecomm
#EPeeps, #EHRA_ESC is proud to have the new 2020 @escardio #AFib guidelines
Here’s my personal #tweetorial about the news and the highlights of these 126 pages.
I congratulate @GerdHindricks, @tanjapotpara1 & whole team for this tremendous work. #ESCGuidelines #EHRA_Ecomm
2/24
Find the new @escardio #Afib guideline document 2020 here ▶️bit.ly/2HD5RKZ.
First, let’s take a look at the "what’s new" part.
Find the new @escardio #Afib guideline document 2020 here ▶️bit.ly/2HD5RKZ.
First, let’s take a look at the "what’s new" part.
3/24
ECG documentation is required to establish the diagnosis of #AFib (either standard 12-lead ECG recording or single-lead ECG tracing of at least 30 s).
I think that this is important because now we can explicitly diagnose AF with single-lead ECGs. #wEHRAbles
ECG documentation is required to establish the diagnosis of #AFib (either standard 12-lead ECG recording or single-lead ECG tracing of at least 30 s).
I think that this is important because now we can explicitly diagnose AF with single-lead ECGs. #wEHRAbles

4/24
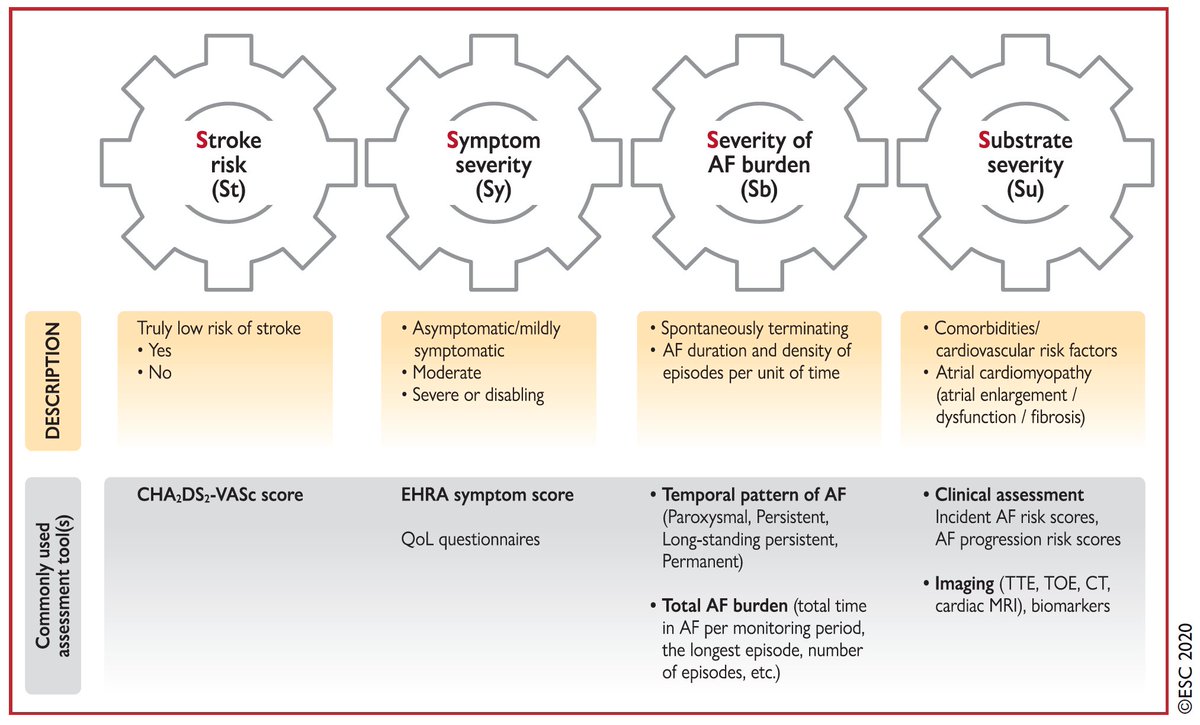
I very much like the new 4S-AF scheme. Very elaborated way to characterize #AFib with an individualized and systematic approach:
Stroke risk: CHA2DS2-VASc
Symptom severity: #EHRA_ESC score
Severity of AF burden: temporal pattern & burden
Substrate severity: clinics & imaging
I very much like the new 4S-AF scheme. Very elaborated way to characterize #AFib with an individualized and systematic approach:
Stroke risk: CHA2DS2-VASc
Symptom severity: #EHRA_ESC score
Severity of AF burden: temporal pattern & burden
Substrate severity: clinics & imaging
5/24
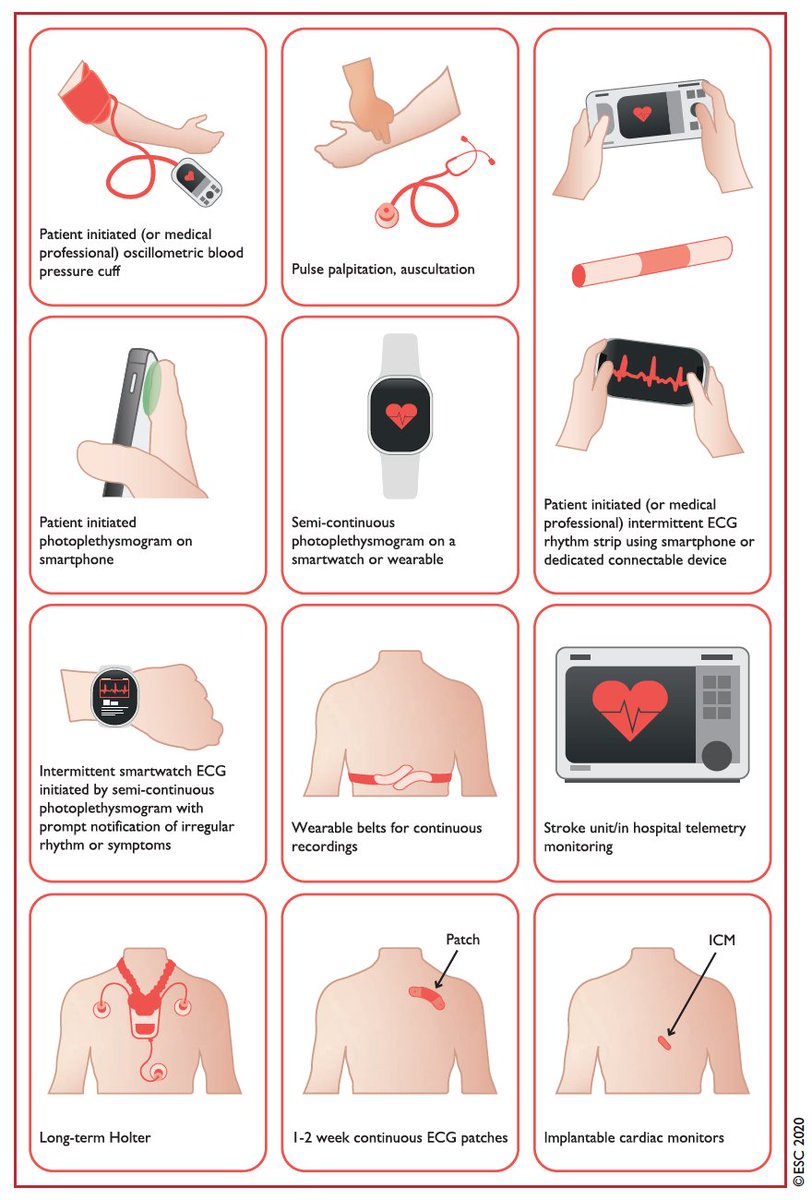
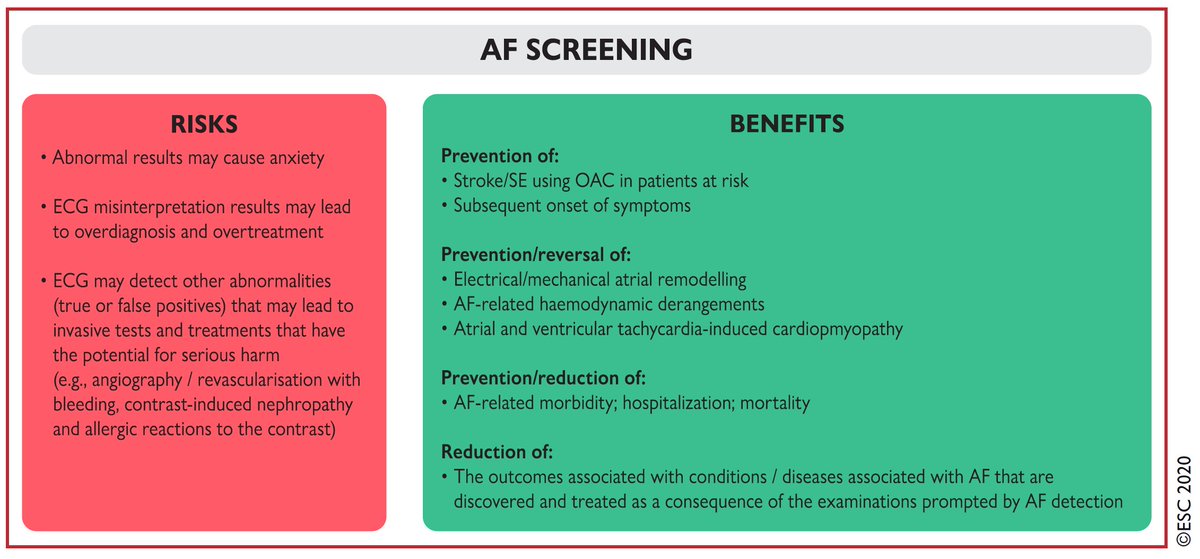
#AFib screening needs to be carefully weighed for pros and cons. We have now a multitude of solutions to screen AF. This myriad of new technologies should not make us forget that overscreening can lead to overdiagnose and overtreatment. Be smart!
#AFib screening needs to be carefully weighed for pros and cons. We have now a multitude of solutions to screen AF. This myriad of new technologies should not make us forget that overscreening can lead to overdiagnose and overtreatment. Be smart!
6/24
Don’t forget patient-reported outcomes (PRO) for #AFib. This now has a ☝️class I recommendation. @Rhythmisit. We need to improve AF management and care from the patient's perspective!
Don’t forget patient-reported outcomes (PRO) for #AFib. This now has a ☝️class I recommendation. @Rhythmisit. We need to improve AF management and care from the patient's perspective!

7/24
Stroke risk does not depend on #Afib classification. Class III indication for clinical pattern of AF conditioning the indication to thromboembolic prophylaxis. A strong message!
Stroke risk does not depend on #Afib classification. Class III indication for clinical pattern of AF conditioning the indication to thromboembolic prophylaxis. A strong message!

8/24
Catheter ablation for PVI is now recommended for rhythm control after 1 failed/intolerant AAD, to improve symptoms of #AFib recurrences in pts w/ parox AF or pers AF w/o or w/ major RF for recurrence.
Look at the quantity of 25 references fortifying this Class I indication!
Catheter ablation for PVI is now recommended for rhythm control after 1 failed/intolerant AAD, to improve symptoms of #AFib recurrences in pts w/ parox AF or pers AF w/o or w/ major RF for recurrence.
Look at the quantity of 25 references fortifying this Class I indication!

9/24
#Afib catheter ablation for PVI should be considered as first-line rhythm control therapy to improve symptoms in selected patients with symptomatic paroxysmal AF episodes (Class IIa).
Poll: What is your main indication for PVI?❓
@escardio @ESC_Journals @ABollmannMD
#Afib catheter ablation for PVI should be considered as first-line rhythm control therapy to improve symptoms in selected patients with symptomatic paroxysmal AF episodes (Class IIa).
Poll: What is your main indication for PVI?❓
@escardio @ESC_Journals @ABollmannMD
10/24
I always wondered why targeting isolation of the pulmonary veins only represented a Class IIa indication in the 2016 guidelines (right panel).
Now, complete electrical isolation of the PV is Class I for all #AFib ablation procedures (left panel). A real improvement!
I always wondered why targeting isolation of the pulmonary veins only represented a Class IIa indication in the 2016 guidelines (right panel).
Now, complete electrical isolation of the PV is Class I for all #AFib ablation procedures (left panel). A real improvement!

11/24
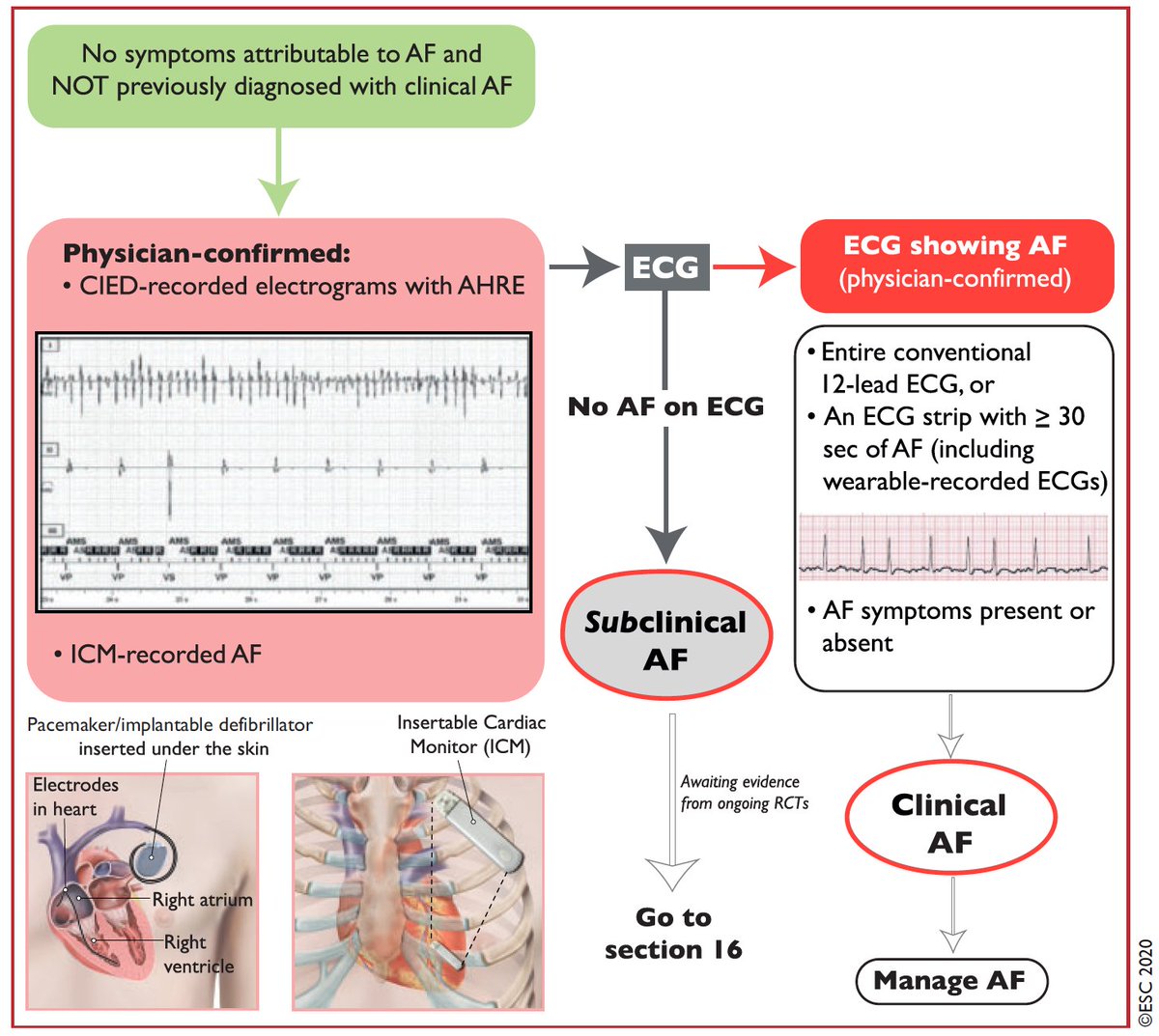
Atrial high rate episodes can be detected by #pacemaker or #ICD with an atrial lead or an insertable cardiac monitor. Always carefully look at the tracings to exclude artifacts and thereby misdiagnosis of #Afib.
Atrial high rate episodes can be detected by #pacemaker or #ICD with an atrial lead or an insertable cardiac monitor. Always carefully look at the tracings to exclude artifacts and thereby misdiagnosis of #Afib.
12/24
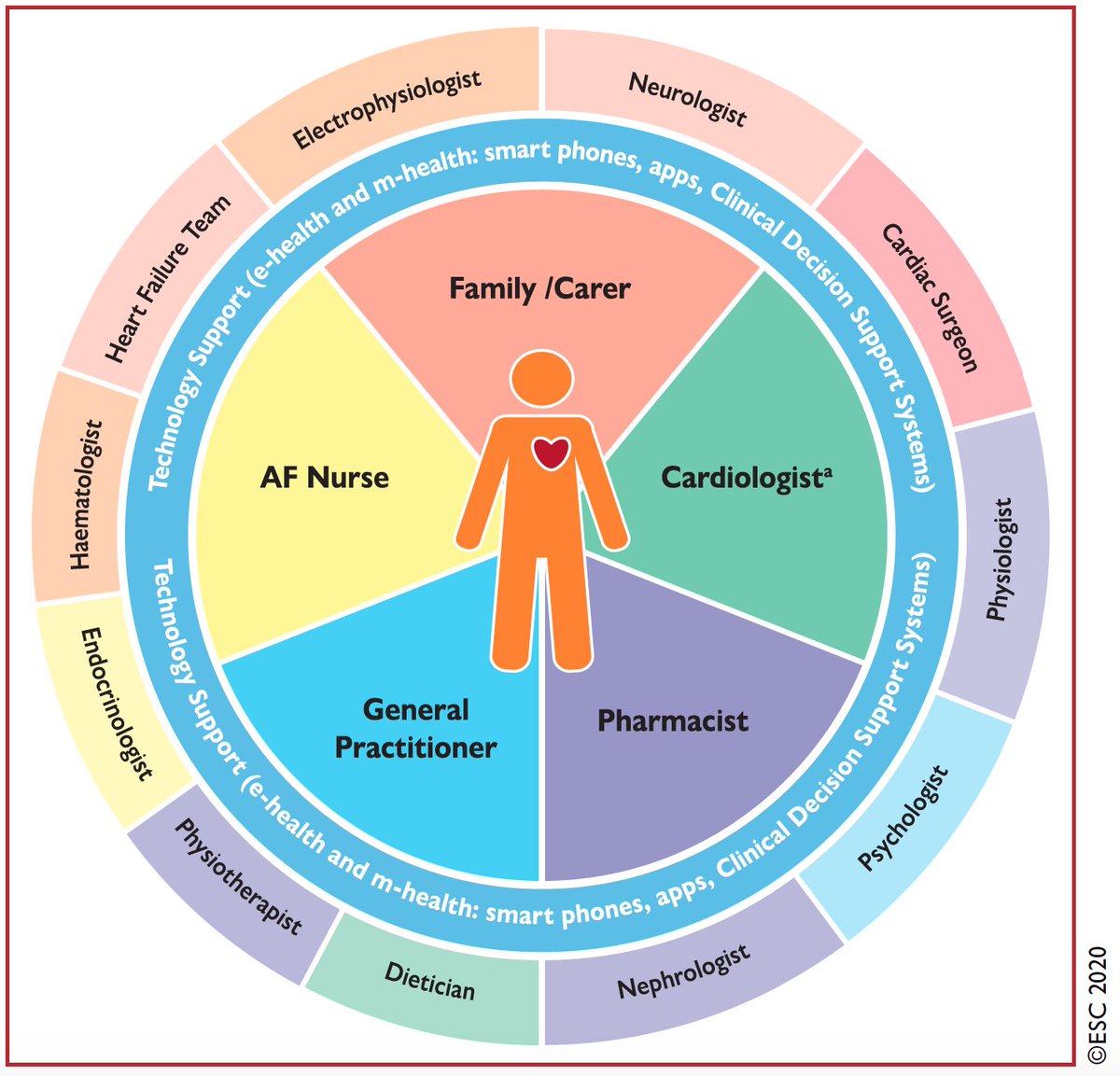
Structured patient management is important for #Afib.
Now comes the new ABC pathway.
Different studies have shown that implementation of the ABC pathway was associated with lower risk of death and CV events.
Structured patient management is important for #Afib.
Now comes the new ABC pathway.
Different studies have shown that implementation of the ABC pathway was associated with lower risk of death and CV events.
13/24
“A” stands for Anticoagulation/Avoid stroke
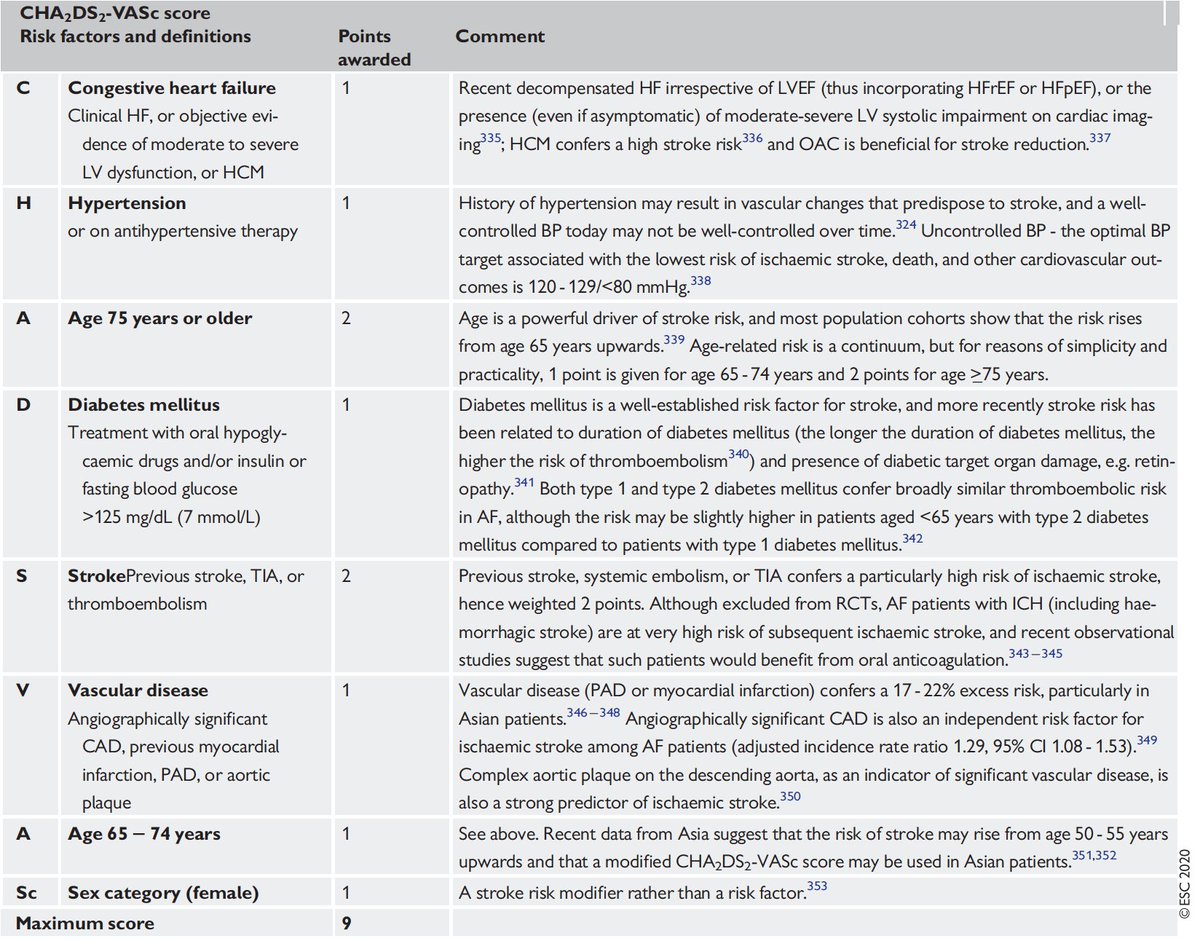
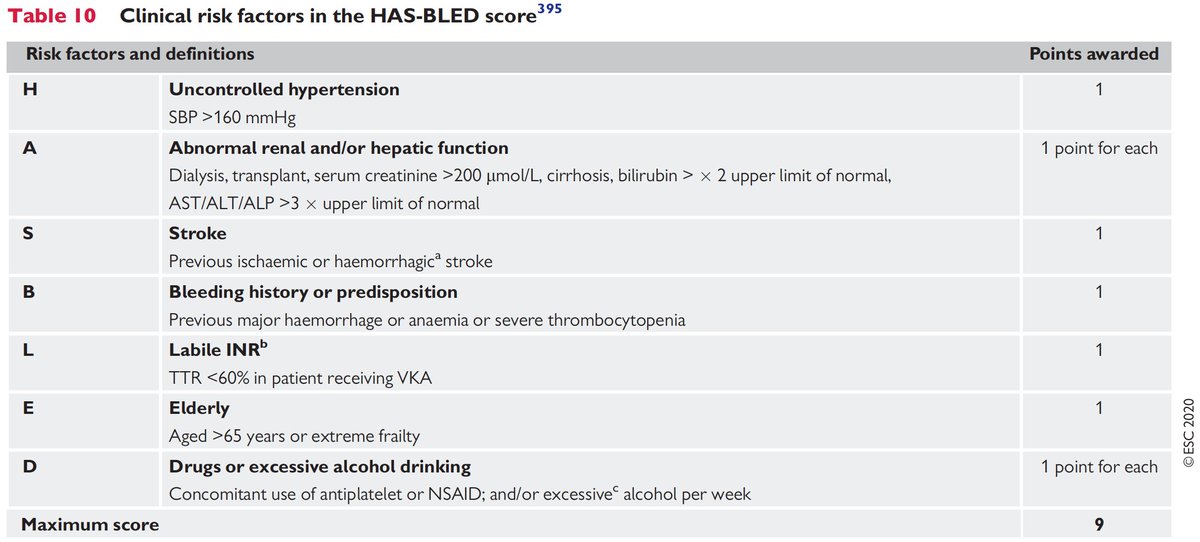
We first need to assess the CHA2DS2-VASc and HASBLED score in #AFib patients.
“A” stands for Anticoagulation/Avoid stroke
We first need to assess the CHA2DS2-VASc and HASBLED score in #AFib patients.
14/24
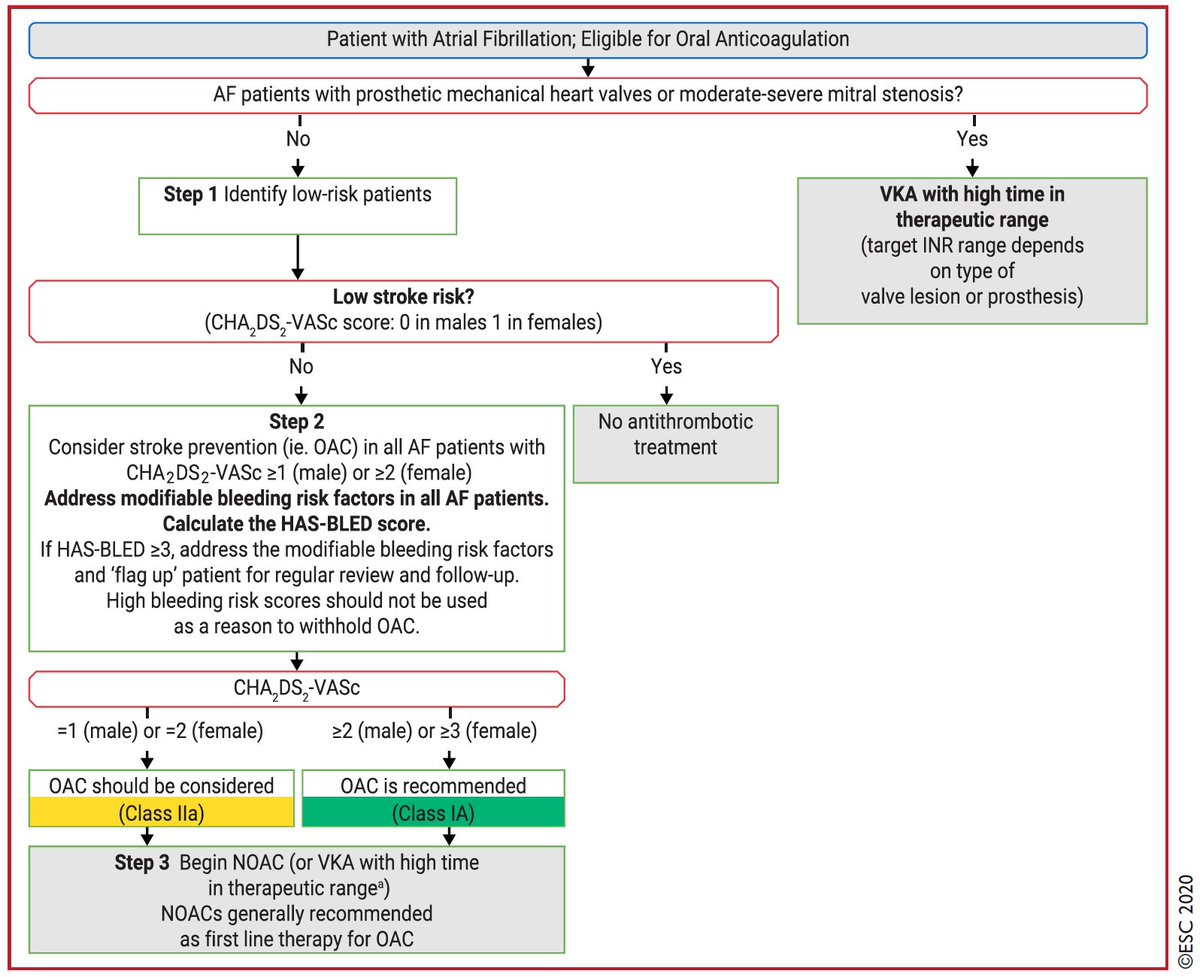
Well-known: oral #anticoagulation should be considered if CHA2DS2-VASc ≥1 in males and ≥2 in females. In patients with #AFib initially at low risk of stroke, first reassessment of stroke risk should be made 4 - 6 months after the index evaluation. A smart recommendation!
Well-known: oral #anticoagulation should be considered if CHA2DS2-VASc ≥1 in males and ≥2 in females. In patients with #AFib initially at low risk of stroke, first reassessment of stroke risk should be made 4 - 6 months after the index evaluation. A smart recommendation!
15/24
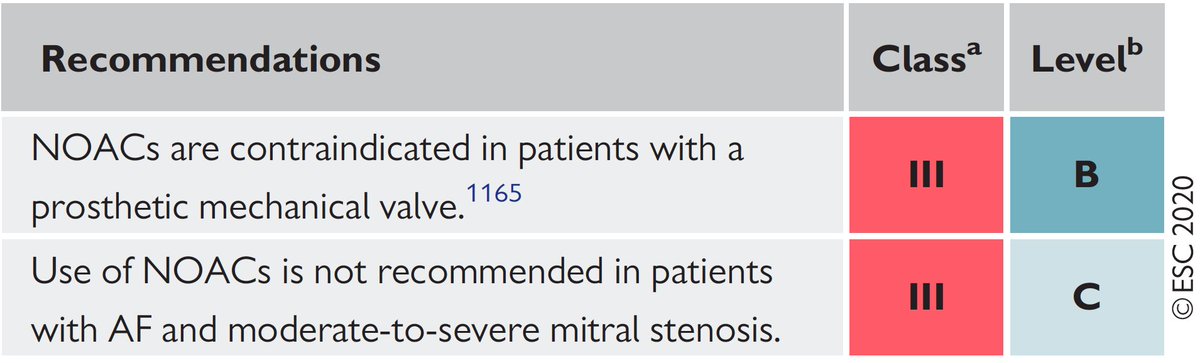
NOACs are the drug of choice for stroke prevention in #Afib.
But don’t forget: Don’t use NOACs in pat with mechanical valves or with moderate-to-severe mitral stenosis!
👀 at the #EHRA_ESC practical guide on NOACs in patients with AF 👉 bit.ly/2FYB0bs
@SteffelJ
NOACs are the drug of choice for stroke prevention in #Afib.
But don’t forget: Don’t use NOACs in pat with mechanical valves or with moderate-to-severe mitral stenosis!
👀 at the #EHRA_ESC practical guide on NOACs in patients with AF 👉 bit.ly/2FYB0bs
@SteffelJ

16/24
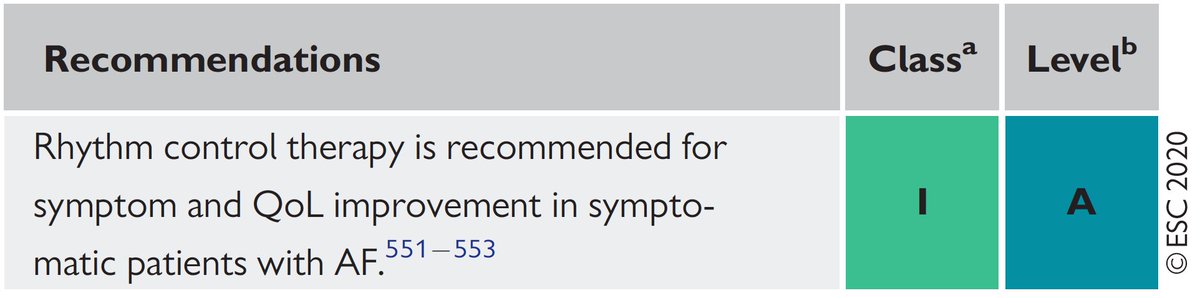
“B” – Better symptom control
Rate or rhythm control? No question: Rhythm control is recommended for symptom and QoL improvement in symptomatic patients with #AFib (Class IA).
“B” – Better symptom control
Rate or rhythm control? No question: Rhythm control is recommended for symptom and QoL improvement in symptomatic patients with #AFib (Class IA).
17/24
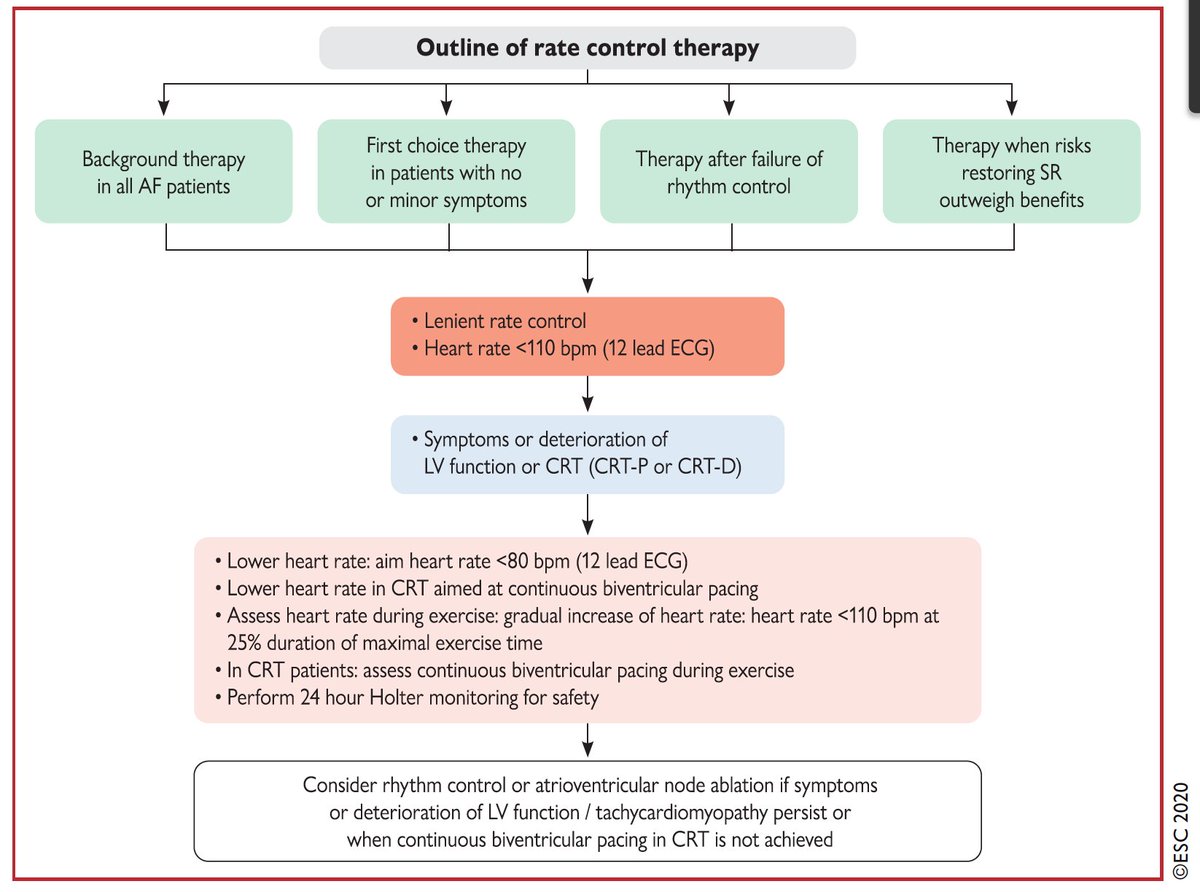
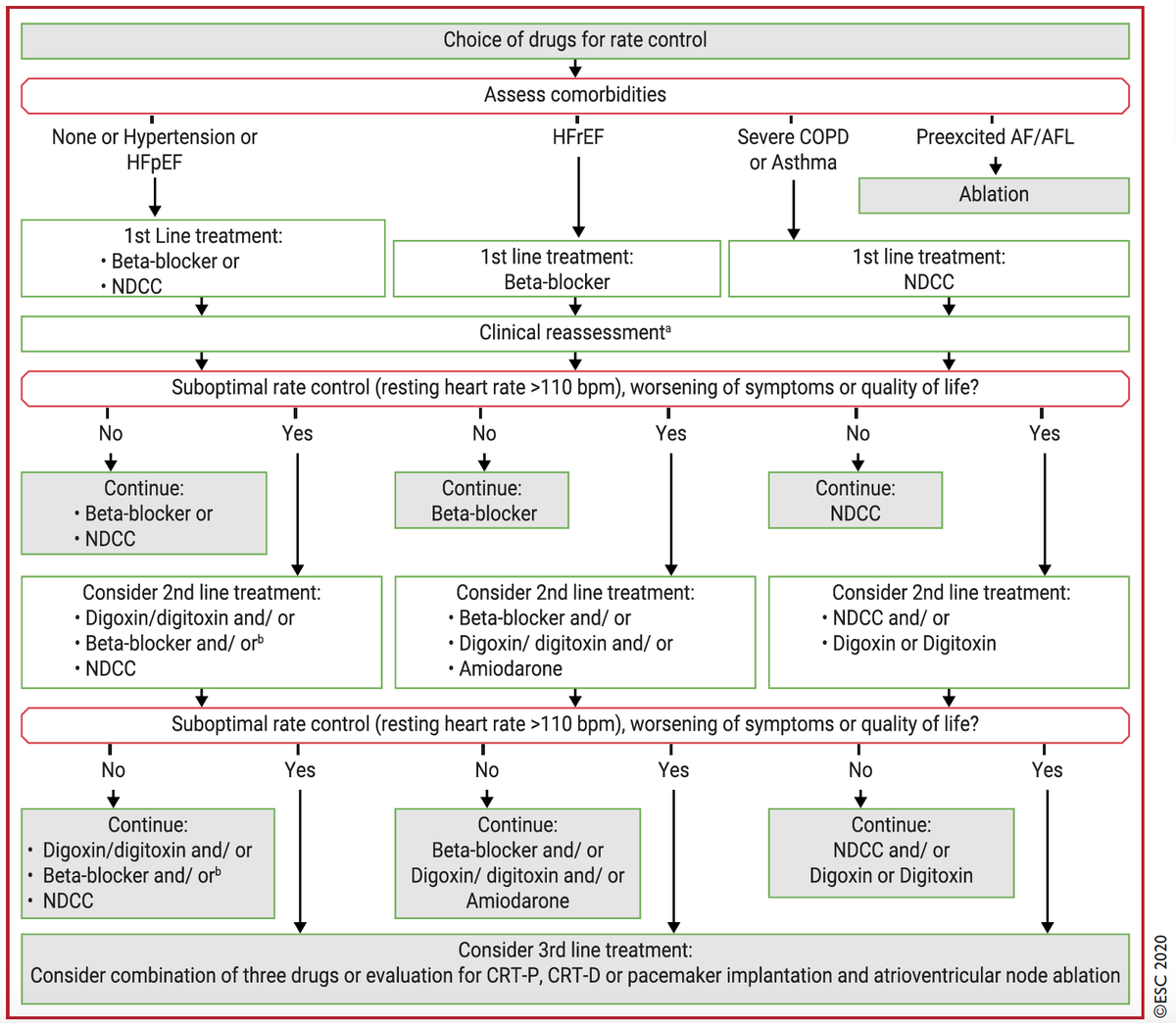
Rate control
For rate control in #Afib: in patients with LVEF≥40%, beta-blockers, diltiazem or verapamil are recommended. In case of LVEF<40%, use beta-blockers or digitalis.
Rate control
For rate control in #Afib: in patients with LVEF≥40%, beta-blockers, diltiazem or verapamil are recommended. In case of LVEF<40%, use beta-blockers or digitalis.
18/24
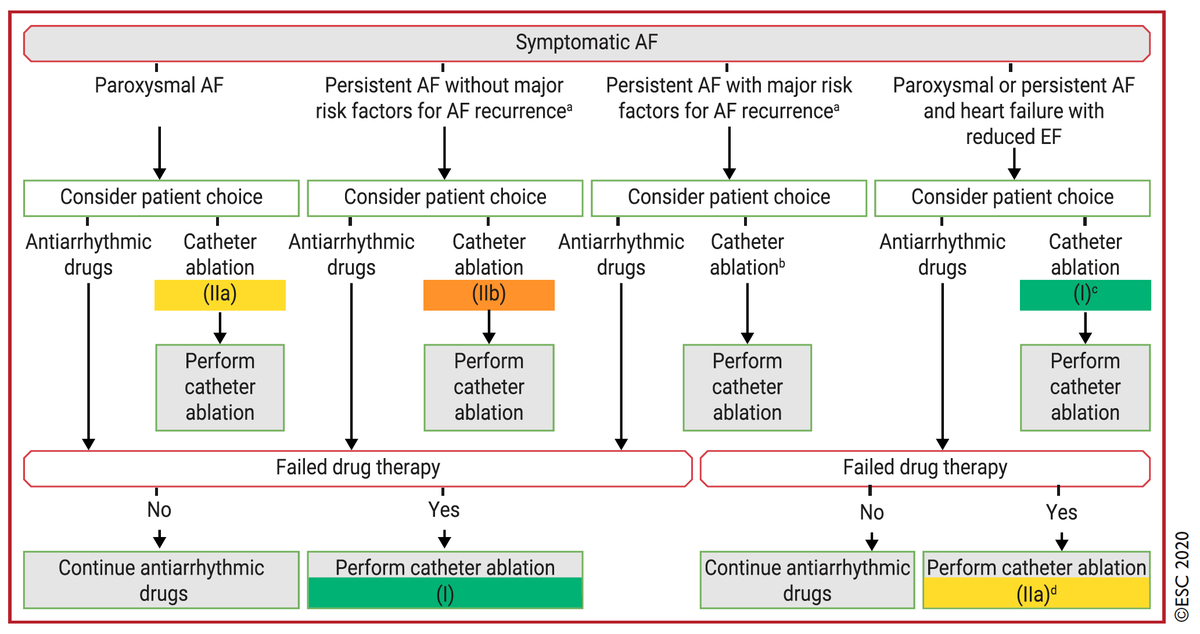
Catheter ablation for symptomatic AF:
It is recommended as 1️⃣line therapy in parox AF (IIa) and persist AF (IIb).
Thanks to the latest data, it is now recommended in tachycardia-induced cardiomyopathy (I) and in pt with ↘️LVEF to ↗️survival and ↘️HF hospitalizations (IIa).
Catheter ablation for symptomatic AF:
It is recommended as 1️⃣line therapy in parox AF (IIa) and persist AF (IIb).
Thanks to the latest data, it is now recommended in tachycardia-induced cardiomyopathy (I) and in pt with ↘️LVEF to ↗️survival and ↘️HF hospitalizations (IIa).
19/24
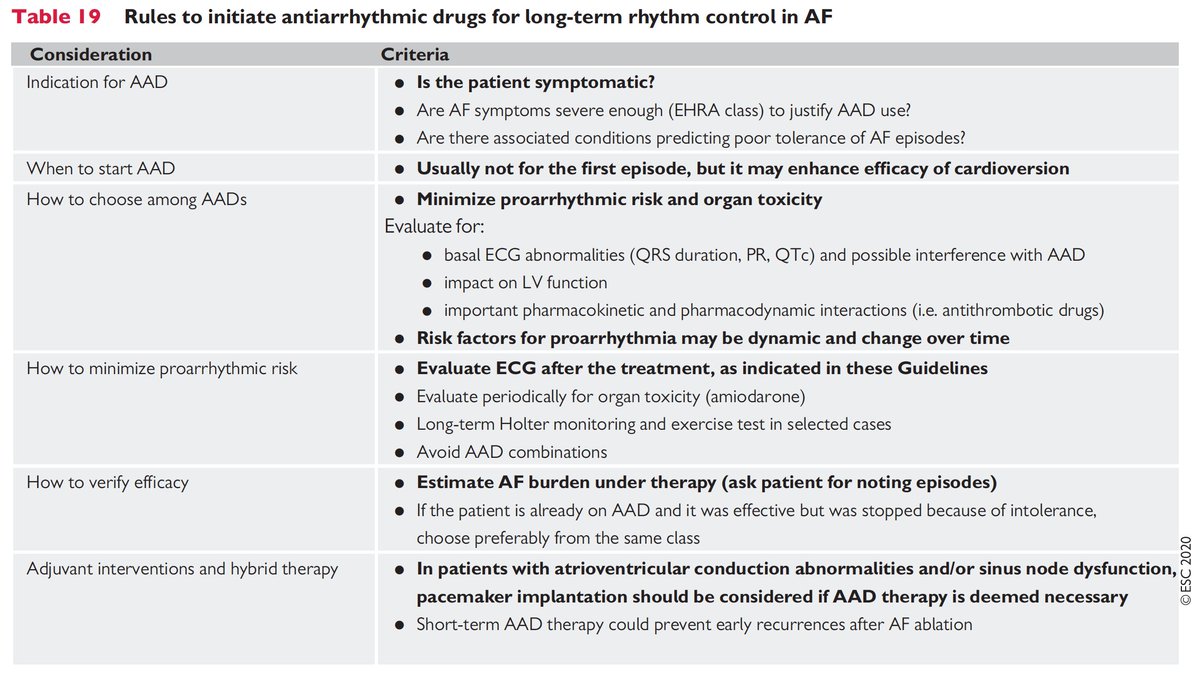
Rules to initiate antiarrhythmic drugs for long-term rhythm control in #Afib.
The first question would be : is my patient symptomatic? Another hint is to redo ECG after treatment initiation!
☝️Re-evaluate and remember PRO!
Rules to initiate antiarrhythmic drugs for long-term rhythm control in #Afib.
The first question would be : is my patient symptomatic? Another hint is to redo ECG after treatment initiation!
☝️Re-evaluate and remember PRO!
20/24
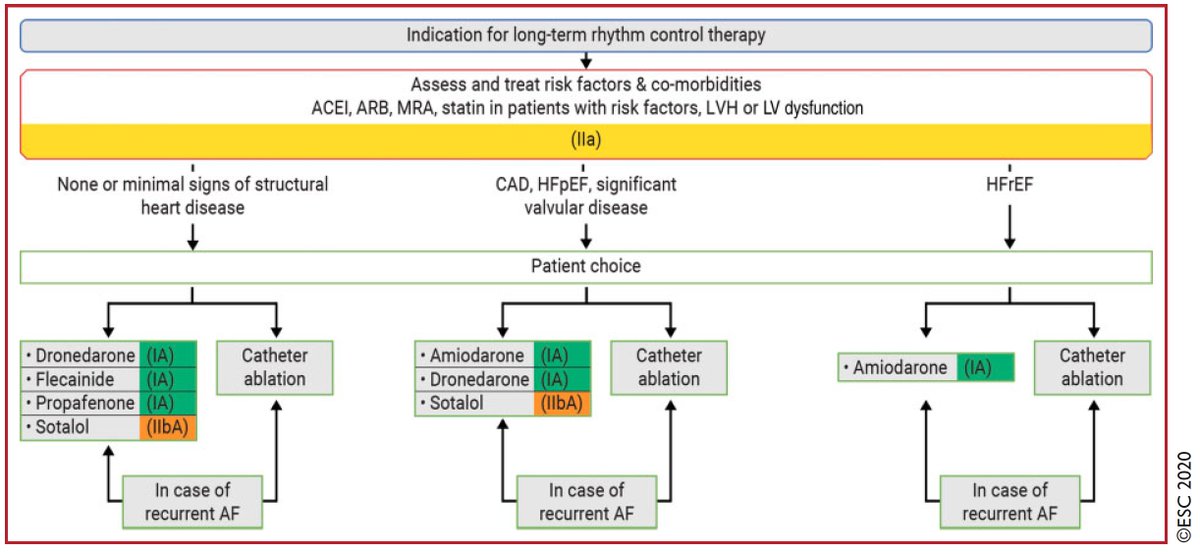
Long-term rhythm control therapy for #Afib.
Patient choice and scientific evidence to be considered!
Remember: close monitoring of QT interval and potassium level are required when using sotalol.
Long-term rhythm control therapy for #Afib.
Patient choice and scientific evidence to be considered!
Remember: close monitoring of QT interval and potassium level are required when using sotalol.
21/24
“C” – Cardiovascular risk factors or concomitant diseases
Or should we call it the 3rd "c"ornerstone for #AFib management?
We need to identify and treat these!
“C” – Cardiovascular risk factors or concomitant diseases
Or should we call it the 3rd "c"ornerstone for #AFib management?
We need to identify and treat these!
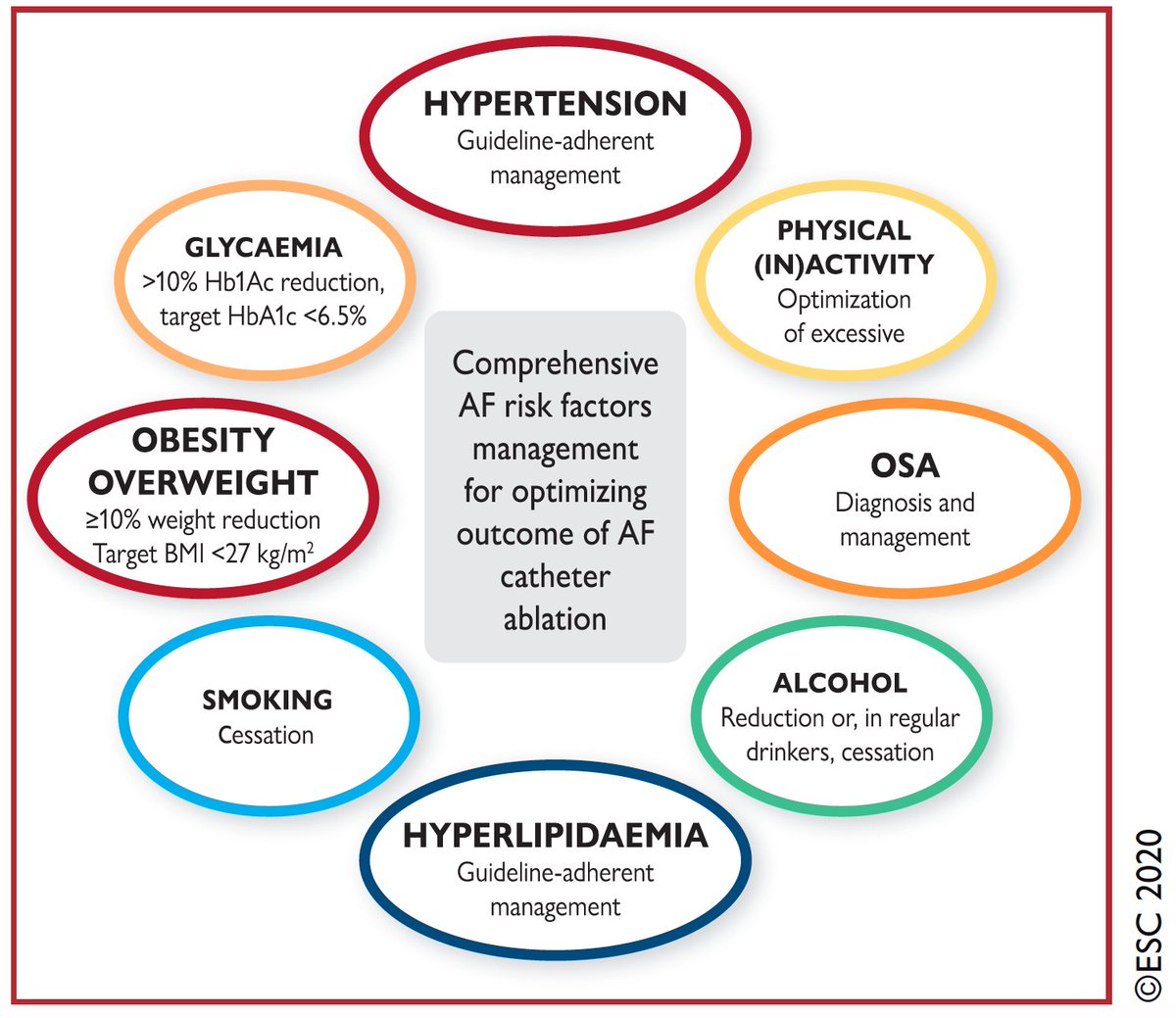
22/24
Identification and management of risk factors and concomitant diseases is recommended as an integral part of treatment in #AFib patients! (Class I)
Poll: Which risk factor do you miss to identify/treat most frequently in your patients?
@PrashSanders @Dominik_Linz
Identification and management of risk factors and concomitant diseases is recommended as an integral part of treatment in #AFib patients! (Class I)
Poll: Which risk factor do you miss to identify/treat most frequently in your patients?
@PrashSanders @Dominik_Linz
24/24
To sum up:
“CC To ABC”
(C)onfirm AF
(C)haracterise AF
(T)reat AF with the ABC pathway
(A) Anticoagulation/Avoid Stroke
(B) Better symptom control
(C) Comorbidities
Thanks for following my first #tweetorial on the new @escardio #Afib guidelines 2020! #EHRA_Ecomm
To sum up:
“CC To ABC”
(C)onfirm AF
(C)haracterise AF
(T)reat AF with the ABC pathway
(A) Anticoagulation/Avoid Stroke
(B) Better symptom control
(C) Comorbidities
Thanks for following my first #tweetorial on the new @escardio #Afib guidelines 2020! #EHRA_Ecomm
• • •
Missing some Tweet in this thread? You can try to
force a refresh


