
A summary of our oral abstract at #kidneywk. Prelim outcomes utilizing both Ellipsys and WavelinQ for #endoavf creations. Compiled and presented by Dr. Genena, one of our fellows. 1/x @ASDINNews #NephTwitter 

Let’s be clear. This isn’t intended as a direct device comparison. This isn’t about if one device is “better.”
These are a compilation of my experiences, thoughts, opinions and limited to my hands only. Yours may be different. That’s ok. Probably preferred. Share and learn. 2/x
These are a compilation of my experiences, thoughts, opinions and limited to my hands only. Yours may be different. That’s ok. Probably preferred. Share and learn. 2/x
It is more of a comparison between the endo-anastomoses. I hypothesized outcomes would be discerned by the location of the anast, so that’s how they are divided and grouped.
Ellipsys: prox RA - perforating vein anast
WavelinQ Ulnar: UA - UV
WavelinQ Radial: prox RA - RV 3/x
Ellipsys: prox RA - perforating vein anast
WavelinQ Ulnar: UA - UV
WavelinQ Radial: prox RA - RV 3/x
This is one user’s experience of many done and to come. This is to foster discussions based on multiple experiences to figure out what makes an endoAVF predictably better and usable. I am still learning. #littlefishbigpond 4/x
1 year of cases, retrospective look, single operator.
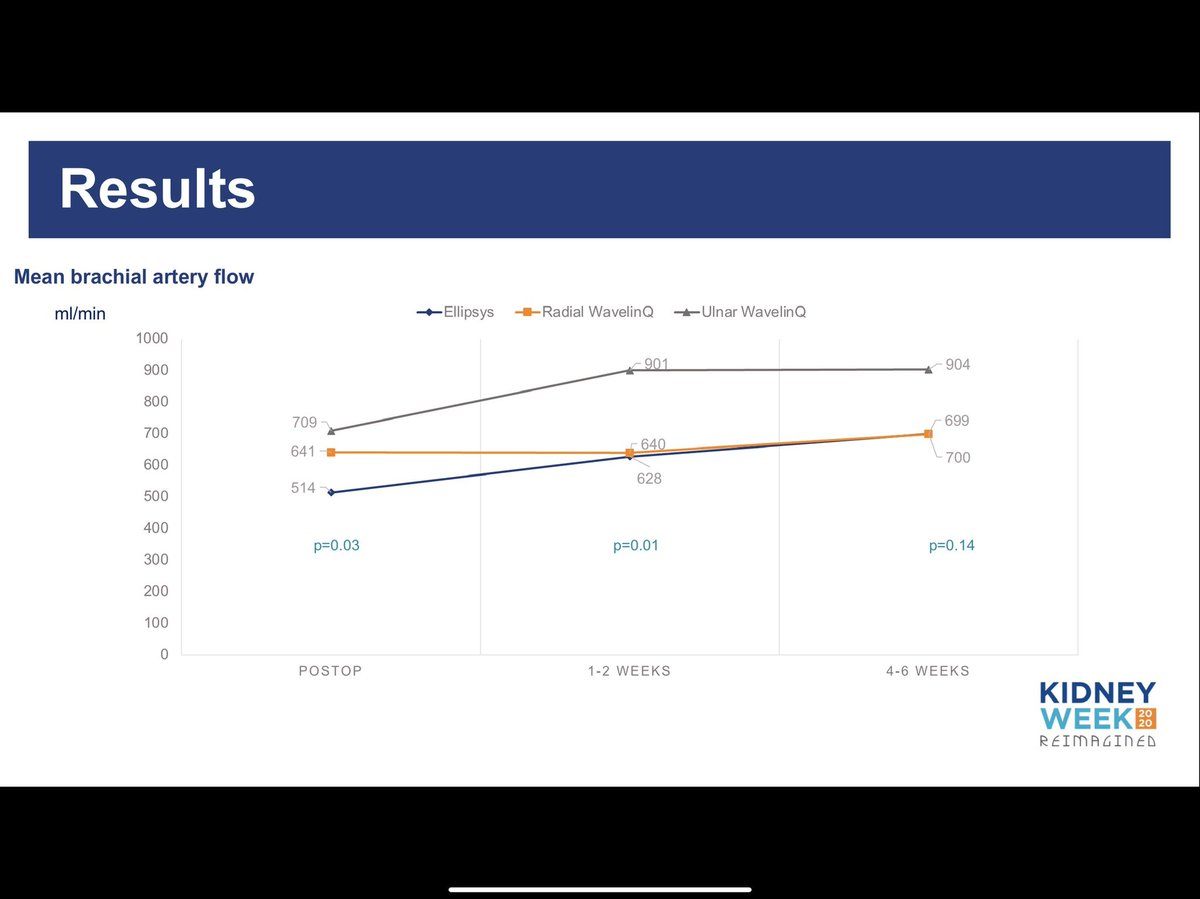
Maturation = Brachial artery flow >500 + AVF vein (ceph and/or median cubital) diameter 5mm. 5/x
Maturation = Brachial artery flow >500 + AVF vein (ceph and/or median cubital) diameter 5mm. 5/x

Numbers aren’t evenly distributed, so absolutely keep that in consideration. I had prior experience in EL and think easier to capture screening, both of which probably played factor here. Also didn’t include unsuccessful cases (learning curves, more for WL). 45% CKD, 70% men. 6/x


Brachial artery flows: Ulnar endo-anastomoses trended higher than a radial endo-anastomoses 7/x
Similar times to maturation, rates of intervention to achieve maturity and to maintain (post maturity) across all three 8/x



Breakdown by the number of total procedures. Most radial anastomoses required maturation or maintenance procedures. 9/x

Number of failures, anywhere from post op visit 1 @ 1-2 weeks to 1 year out. These do not translate into patency rates. Most failed due to a juxta-anastomotic vein stenosis. 10/x

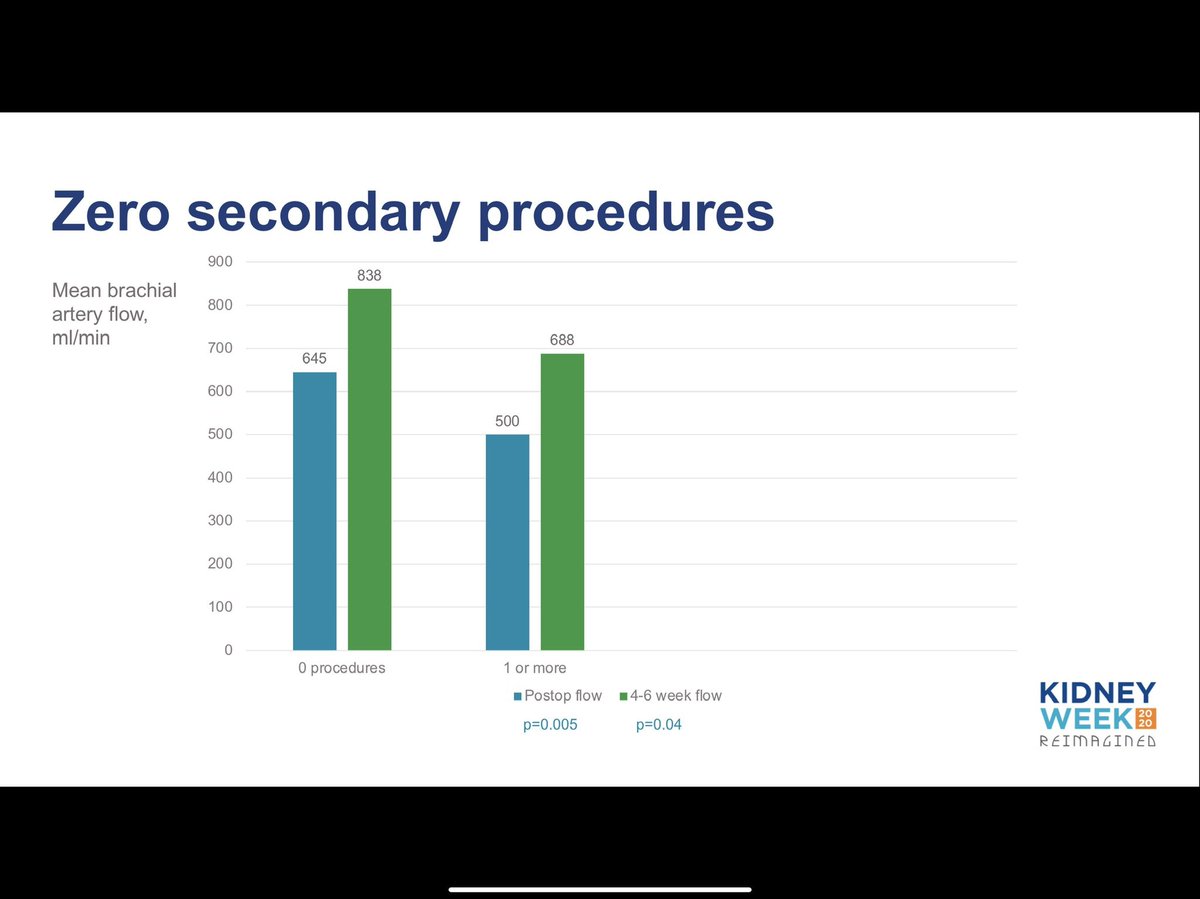
Higher brachial artery flows correlated with fewer maturation procedures required regardless (or irregardless 😂) of endo-anastomosis. 11/x
Men did better than women. Fewer failures. But is it because of gender or higher flows? 12/x


So it seems like higher brachial artery flows fared better - fewer interventions and fewer failures. Ulnar anastomoses and men tended to have higher brachial artery flows. I see this as the focus - how do I optimize (?maximize) brachial artery flows? 13/x


And if you want to ask me which device to use, my answer always is:
Both.
An endoAVF practice should have both devices in house to offer your patients.
If you don’t carry only 1 brand of PC, stent, balloon, etc - don’t tell me you only need 1 brand for #endoAVF #pavf /X
Both.
An endoAVF practice should have both devices in house to offer your patients.
If you don’t carry only 1 brand of PC, stent, balloon, etc - don’t tell me you only need 1 brand for #endoAVF #pavf /X
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh


