
Folks always confuse 1:1,000 vs. 1:10,000 epinephrine, when you're supposed to use which, what the dosing is, etc
Here's what helps me remember/teach.
Thread 1/9
Here's what helps me remember/teach.
Thread 1/9
There's two main indications for epi - code blue and anaphylaxis.
1. Code blue is a 1mg IV dose of 1:10,000 epi
2. Anaphylaxis is 0.3mg IM dose of 1:1,000 epi
Shouldn't be that hard to remember... but it is.
2/
1. Code blue is a 1mg IV dose of 1:10,000 epi
2. Anaphylaxis is 0.3mg IM dose of 1:1,000 epi
Shouldn't be that hard to remember... but it is.
2/
There's the route, the dose, and the concentration.
The route is easiest. Think of epi being pushed IV during a code. Think of the epipen people jab into their thigh muscle for anaphylaxis.
1. Code – IV
2. Anaphylaxis - IM
Great, moving on.
3/
The route is easiest. Think of epi being pushed IV during a code. Think of the epipen people jab into their thigh muscle for anaphylaxis.
1. Code – IV
2. Anaphylaxis - IM
Great, moving on.
3/
Next the dose. Got a mnemonic for that too.
A code is worse than anaphylaxis so you need a bigger dose of epi.
1. Code - 1 mg
2. Anaphylaxis - 0.3 mg
Cool.
4/
A code is worse than anaphylaxis so you need a bigger dose of epi.
1. Code - 1 mg
2. Anaphylaxis - 0.3 mg
Cool.
4/
Now the formulation, which is the most confusing.
The secret is knowing what the 1:10,000 and 1:1,000 mean.
These units are mg (of epi) per MICROliter (of water).
Unfortunately we don’t think in microliters, we think in milliliters...
5/
The secret is knowing what the 1:10,000 and 1:1,000 mean.
These units are mg (of epi) per MICROliter (of water).
Unfortunately we don’t think in microliters, we think in milliliters...
5/
Luckily the conversion is easy. One mL is 1000 mcL. So just dropping three zeroes starts to make a lot of sense:
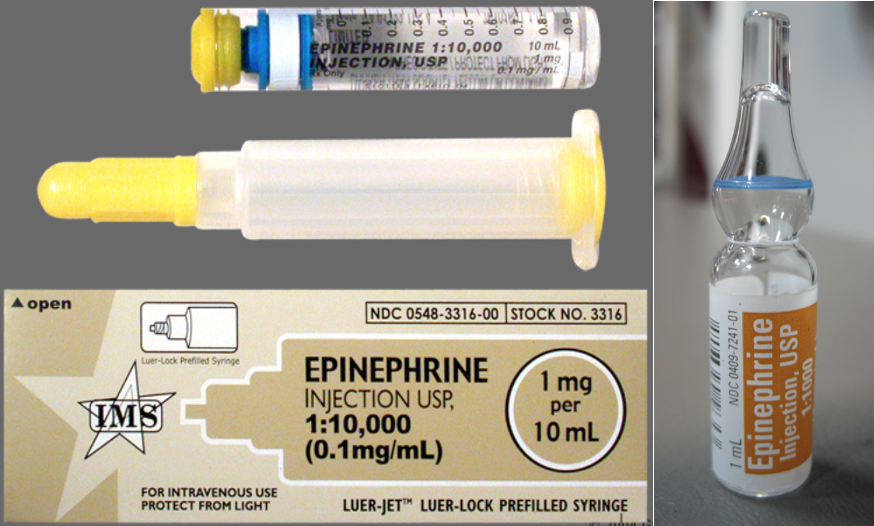
It's why 1:10,000 comes as a 10 mL stick, and 1:1,000 is a 1 mL ampule.
1.Code 1:10 mg:mL
2.Anaphylaxis 1:1 mg:mL
6/
It's why 1:10,000 comes as a 10 mL stick, and 1:1,000 is a 1 mL ampule.
1.Code 1:10 mg:mL
2.Anaphylaxis 1:1 mg:mL
6/

So for IV (code) it’s the more dilute solution, and for IM (anaphylaxis) it’s the more concentrated solution.
Which makes sense if you think about it… you don’t want to be injecting multiple mL of fluid into muscle, a big ole bubble of fluid won't absorb as well.
7/
Which makes sense if you think about it… you don’t want to be injecting multiple mL of fluid into muscle, a big ole bubble of fluid won't absorb as well.
7/
In summary:
1. Code: take the whole 10 mL stick of 1:10 mg/mL epi (1mg) and inject it IV
2. Anaphylaxis: draw up about 1/3 of the 1mL ampule of 1:1 mg/mL epi (0.3mg) and inject it IM
8/
1. Code: take the whole 10 mL stick of 1:10 mg/mL epi (1mg) and inject it IV
2. Anaphylaxis: draw up about 1/3 of the 1mL ampule of 1:1 mg/mL epi (0.3mg) and inject it IM
8/
When you forget, just ask:
1. Wait which one is IM? Epipen! Anaphylaxis
2. What does 1:1000 mean? Drop 0s. 1mg in 1mL... as opposed to in 10mL. So 1:1 more concentrated. Better for IM.
2. What's the dose for anaphylaxis? Not as bad as code, so less than 1mg. Oh it's 0.3!
9/9
1. Wait which one is IM? Epipen! Anaphylaxis
2. What does 1:1000 mean? Drop 0s. 1mg in 1mL... as opposed to in 10mL. So 1:1 more concentrated. Better for IM.
2. What's the dose for anaphylaxis? Not as bad as code, so less than 1mg. Oh it's 0.3!
9/9
Some people brought up dosing of 0.5 mg IM for anaphylaxis.
Newest guidelines (tinyurl.com/ybrsqcea) recommend 0.01 mg/kg up to 0.5 mg, so indeed 0.5 for adults >50kg.
Epipens are still 0.3 mg.
But agreed, if drawing up epi ourselves, 0.5 mg appropriate for most adults.
Newest guidelines (tinyurl.com/ybrsqcea) recommend 0.01 mg/kg up to 0.5 mg, so indeed 0.5 for adults >50kg.
Epipens are still 0.3 mg.
But agreed, if drawing up epi ourselves, 0.5 mg appropriate for most adults.
• • •
Missing some Tweet in this thread? You can try to
force a refresh





