The experts and references say IgE-mediated anaphylaxis is vanishingly rare. Good.
Most IV iron reactions are thought to be complement-activation-related pseudo-allergy, the final effect of which is histamine release.
Why does this preclude serious reactions?
2/6
Aug 4, 2023 • 5 tweets • 1 min read
Infection is one of the most common causes of hypotension, right? Right.
Imagine a patient in the hospital who has an infection. His BP is 80/50. He’s lying there, tired, a bit lightheaded.
1/4
We give him 1000 cc LR. His BP improves to 110/60, and he is no longer dizzy.
But the he gets up to use the restroom, and he feels dizzy again. Because gravity just subtracted most of that bolus we gave him into his legs.
2/
Apr 17, 2023 • 11 tweets • 2 min read
How do salt tabs and urea work in treating SIADH?
They force you to excrete water that you otherwise wouldn't have excreted.
1/
A puzzle:
If this statement is true...
"You can either fluid restrict to 1 liter, or fluid restrict to 1.5 liters AND take 3 one-gram salt tabs with every meal, and achieve the same result"
That must mean that the urine osmolarity is...
2/
Jan 18, 2023 • 14 tweets • 4 min read
Ultrasound: “no evidence of cholecystitis”
Op report: “gangrenous cholecystitis with extremely friable tissue. Purulent drainage with manipulation of gallbladder.”
I've seen this many times.
Thread
1/
Like any test, RUQUS is not perfect in detecting cholecystitis.
A systematic review in 2012 put pooled sensitivity at 81%, but as you see in plot of included studies, there's heterogeneity, with sensitivity as low as 50% in some studies.
Will be referring to these during a basic POCUS workshop where learners practice scans on normal volunteers.
Non-scanning learners can pull up and show some abnormal examples in parallel with live demo of normal findings
00 - Normal parasternal long-axis (PLAX) view
Mar 4, 2022 • 5 tweets • 1 min read
Let's play a little fremitus game, just for fun:
Press the hypothenar edge of your hand firmly against your own ribcage. You're gonna keep it there the whole time while you say some stuff and feel the amount of vibrations transmitted.
Let's go.
1/5
Experiment # 1:
Compare the amount of fremitus/vibration when you say:
ninety-nine
noy-noy-noy
one-two-three
Feel free to repeat a couple times.
Did any of them cause more vibration than others?
2/5
Nov 1, 2021 • 9 tweets • 2 min read
If you eat yourself, will you get hyperkalemic?
Sorry, let me rephrase:
Can upper GI bleeding cause hyperkalemia in predisposed people?
I feel like I’ve gotten that vibe from a couple patients. I can’t find any reports from others.. but I can think of a mechanism...
1/
Blood contains a lot of protein.
When a significant amount of it is introduced into the proximal GI lumen (and some of it absorbed), it can elevate your BUN, or trigger hepatic encephalopathy.
2/
Sep 7, 2021 • 5 tweets • 2 min read
Many medicine procedures involve (1) pushing a needle into a fluid-filled space, (2) advancing a plastic catheter over the needle into the space, (3) pulling the needle out, and (4) leaving the catheter in either for drainage or infusion.
Things often go wrong at (2).
1/5
When you first get a “flash” (enter the fluid filled space with your needle), only the very tip/distal part of the needle/bevel is in the target space.
Let’s use paracentesis as an example.
In these photos, the paper is the peritoneum, with views from both sides of it.
2/
Aug 9, 2021 • 10 tweets • 2 min read
I was taught, and continue to hear it taught, that the history of present illness (HPI) should be crafted to "convince the listener/reader of your suspected diagnosis."
I think this framing is problematic...
1/
The HPI should outline the patient's experience of illness chronologically, and include with some neutrality details relevant to the *differential* diagnosis.
As well as those symptoms particularly emphasized by the patient (in case you aren't thinking of all differentials).
2/
May 25, 2021 • 18 tweets • 8 min read
This was an MI of the RV + inferior LV, with complete heart block, caused by a thrombotic occlusion of the proximal RCA.
Thanks all for commenting. 🧵 below has some basic stuff + nerdy stuff, hopefully something helpful for everyone.
Had a cleaning a couple weeks ago, she said I had a small cavity worth filling. I went back today to do that.
1/5
She pokes around, makes eyebrows, says let me go look at that X-ray again.
Pokes around some more, pauses for a moment.
“Let’s just leave it alone and watch it.”
2/
Jan 2, 2021 • 5 tweets • 2 min read
The difference between comic books and the New Yorker magazine cartoons/captions: why chronology is critical in clinical history and diagnosis.
1/5
In the New Yorker cartoon and caption contest, a single still frame of a scene is presented.
Even if the scene has a lot of detail, hundreds of possible interpretations and realities are imagined/solicited.
2/5
Dec 7, 2020 • 13 tweets • 3 min read
As you turned the corner on the second flight of stairs, you felt your breath pull a little deeper, the next one come a little earlier. Your heart said 👋🏼, bounding softly in your neck.
Ten seconds down the hall, all that faded. You were back to mulling some thought.
1/
But hold on. Let’s pause for a minute and retrace the steps.
A lot happened before the extra breath and the tug in your neck caught your attention.
And it’s all so damn cool.
2/
Nov 27, 2020 • 7 tweets • 3 min read
I’m fascinated by the question raised in this great blog post (read first).
I’ve always thought of severe hypertension as a cause of increased myocardial oxygen demand. Which makes sense for the SBP (afterload, wall stress)... it’s what the LV is contracting against.
2/
Nov 11, 2020 • 10 tweets • 3 min read
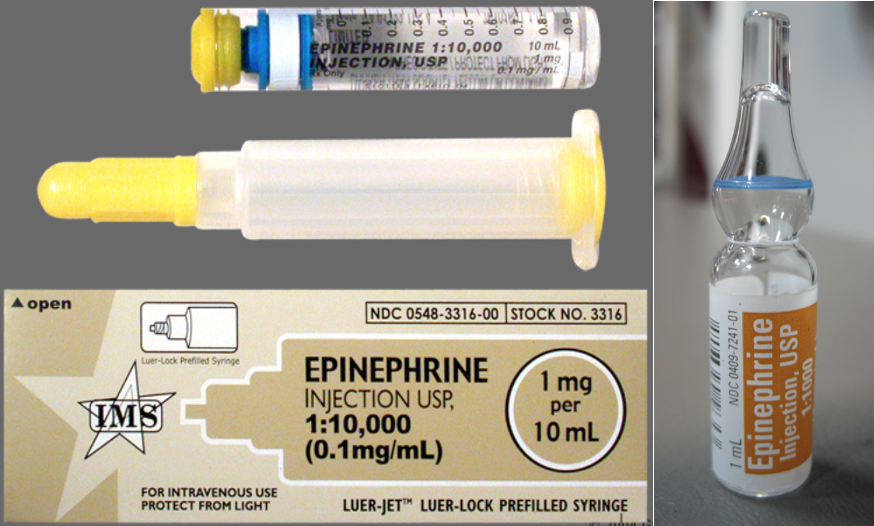
Folks always confuse 1:1,000 vs. 1:10,000 epinephrine, when you're supposed to use which, what the dosing is, etc
Here's what helps me remember/teach.
Thread 1/9
There's two main indications for epi - code blue and anaphylaxis.
1. Code blue is a 1mg IV dose of 1:10,000 epi
2. Anaphylaxis is 0.3mg IM dose of 1:1,000 epi
Shouldn't be that hard to remember... but it is.
2/
Oct 1, 2020 • 6 tweets • 2 min read
Descriptive terms are great.
Take “calcific uremic arteriopathy.”
Arteriopathy. There’s a problem with arteries, so you might guess manifestations may be ischemic/necrotic.
1/6
Calcific...
Calcium deposits in the arteriolar walls, usually of the skin, causing fibrosis, thrombosis, obstruction.
Uremic...
This usually happens in the setting of kidney disease and a high calcium-phosphate product, though it’s complicated.
PMID 29719190
2/
Sep 15, 2020 • 6 tweets • 2 min read
+1 for organization/structure as foundation of effective communication.
Learners often struggle with shifting expectations. And teachers sometimes associated highly structured presentations with wordy ones. So I want to emphasize:
First, our own practice & quality of care suffer when we think in extremes and absolutes.
Second, we can communicate oversimplified or wrong messages to learners who don’t have the same contextual knowledge.
Some examples of such misunderstandings...
2/
Sep 3, 2020 • 4 tweets • 1 min read
Had a realization about quiet heart sounds that came about a decade late.
Short thread.
1/4
Ok.
S1 and S2 happen when pressure gradients snap them shut. Right-sided cardiac pressures and thus valve-closing pressure gradients are lower, this P2 is quieter than A2.
And if you get pulmonary hypertension, P2 gets louder.
A bit more from UpToDate:
2/4
Jul 25, 2020 • 9 tweets • 4 min read
I haven’t ordered a CK-MB in 8 years.
If you’re worried about the ❤️, it adds nothing to your troponin.
If you’re worried about 🥩💪🏽, it adds nothing to CK.
Many hospital/labs don’t even run CK-MBs, considering them too low-value.
#TipsForNewDocs
Thanks for comments, y’all. Regarding utility in detecting reinfarction:
First, I must say that I do hospital medicine and minimal ICU, so this isn’t a daily quandary for me. I was mostly imagining the “new docs” on the wards.