1/
#EHRA_ESC tweetorial on anticoagulation & stroke prevention.
#EPeeps, after having done an overview #tweetorial on the new @escardio #AFib guidelines 2020 👉bit.ly/2ITAbCq, I will go more in depth into several topics of these guidelines in the next weeks
#EHRA_Ecomm
#EHRA_ESC tweetorial on anticoagulation & stroke prevention.
#EPeeps, after having done an overview #tweetorial on the new @escardio #AFib guidelines 2020 👉bit.ly/2ITAbCq, I will go more in depth into several topics of these guidelines in the next weeks
#EHRA_Ecomm

2/
Find the first @escardio guidelines on #afib 2020 tweetorial here
👉
#EHRA_ESC #EHRA_Ecomm
Find the first @escardio guidelines on #afib 2020 tweetorial here
👉
https://twitter.com/EHRAPresident/status/1320648874571300864?s=20
#EHRA_ESC #EHRA_Ecomm

3/
I think that this figure which summarizes OAC in #AFib is very didactic and practical. Please note that NOACS are generally recommended as first line therapy for OAC.
@tanjapotpara1 @GerdHindricks @SteffelJ
I think that this figure which summarizes OAC in #AFib is very didactic and practical. Please note that NOACS are generally recommended as first line therapy for OAC.
@tanjapotpara1 @GerdHindricks @SteffelJ

4/
Very important:
even if the risk of ischaemic stroke is higher with persistent #AFib compared to paroxysmal, the temporal pattern should not affect the decision regarding long-term OAC.
Very important:
even if the risk of ischaemic stroke is higher with persistent #AFib compared to paroxysmal, the temporal pattern should not affect the decision regarding long-term OAC.

5/
Patients with prosthetic mechanical heart valve or moderate to severe mitral stenosis are indicated for VKA, not NOACs. Be careful!
Also remember the #EHRA_ESC practical guide on NOACs: ✍️bit.ly/2JN5Rda
@SteffelJ
Patients with prosthetic mechanical heart valve or moderate to severe mitral stenosis are indicated for VKA, not NOACs. Be careful!
Also remember the #EHRA_ESC practical guide on NOACs: ✍️bit.ly/2JN5Rda
@SteffelJ

6/
Calculate the CHA2DS2-VASc score. This is critical and is often not well performed. For example, the C letter not only stands for #HeartFailure but also asymptomatic LV dysfunction or hypertrophic cardiomyopathy.
Calculate the CHA2DS2-VASc score. This is critical and is often not well performed. For example, the C letter not only stands for #HeartFailure but also asymptomatic LV dysfunction or hypertrophic cardiomyopathy.

7/
Identify patients at low stroke risk i.e. patients with CHA2DS2-VASc score 0 for men and 1 for women.
🚫These patients do not require OAC.
But a periodic revaluation is recommended.
Identify patients at low stroke risk i.e. patients with CHA2DS2-VASc score 0 for men and 1 for women.
🚫These patients do not require OAC.
But a periodic revaluation is recommended.

8/
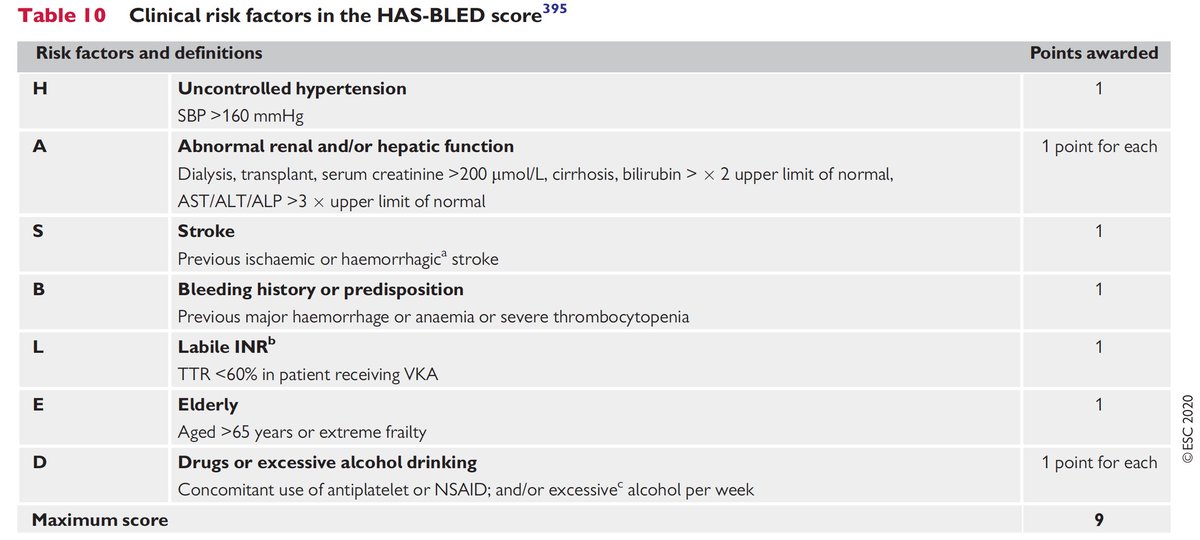
Calculate the HAS-BLED score to identify patients with a high bleeding risk.
High bleeding risk is determined when HAS-BLED ≥3.
All modifiable risk factors of bleeding should be addressed.
🛠 bit.ly/379Bh62
Calculate the HAS-BLED score to identify patients with a high bleeding risk.
High bleeding risk is determined when HAS-BLED ≥3.
All modifiable risk factors of bleeding should be addressed.
🛠 bit.ly/379Bh62
9/
Then anticoagulate!✅
It's a Class IIa indication in patients with CHA2DS2-VASc score =1 in males and 2 in females
and a Class IA indication if the score is ≥2 in males and ≥3 in females.
Then anticoagulate!✅
It's a Class IIa indication in patients with CHA2DS2-VASc score =1 in males and 2 in females
and a Class IA indication if the score is ≥2 in males and ≥3 in females.


• • •
Missing some Tweet in this thread? You can try to
force a refresh