According to the new CBO report, under single-payer, we could cover ~100% of the population, make medical services free at point of use, and expand benefits — without spending a dollar more. And healthcare providers would still do perfectly well. 
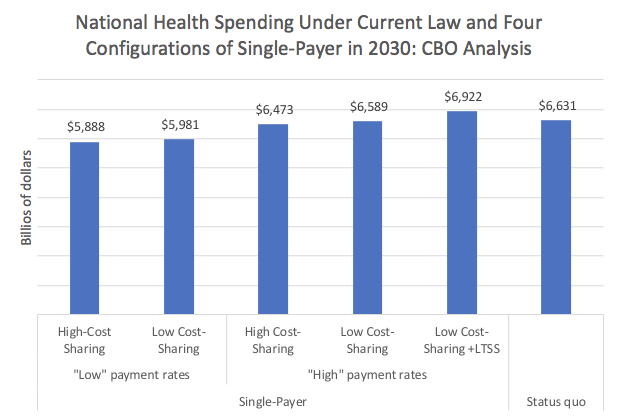
If you also add, as we should, universal long term care with no out-of-pocket costs, you'd spend about ~$300 billion more a year on healthcare altogether, they estimate — but we'd have a free-at-point-of-use system with comprehensive benefits for all, including long-term care.
I'll have many more thoughts on this analysis soon, but the bottom line is clear.
Any healthcare reform other than single-payer will either have higher costs or skimpier benefits than single-payer.
Any healthcare reform other than single-payer will either have higher costs or skimpier benefits than single-payer.
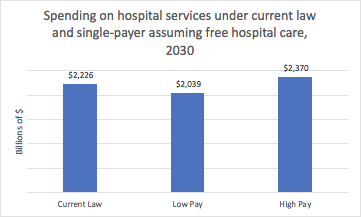
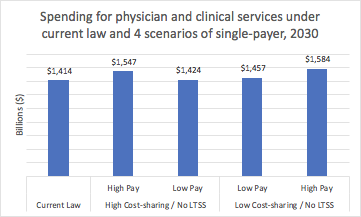
(To clarify axis labels, “low cost-sharing” = no copays/deductibles for any health services and low cost-sharing for drugs; “high cost-sharing” is some cost-sharing but less than status quo; “payments” refers to doctor/ hospital payments; LTSS=long term services and supports).
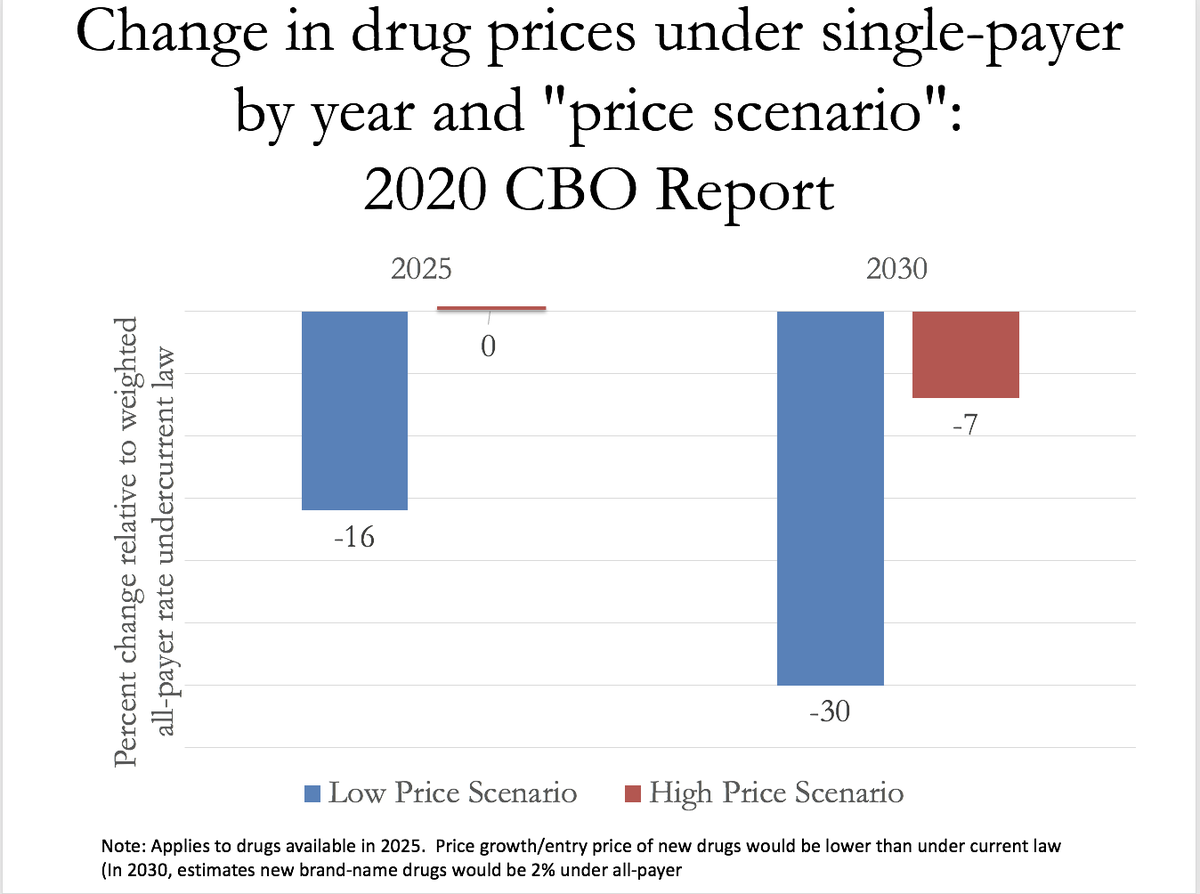
For now, will note CBO makes v. modest assumptions about drug price reductions under single-payer. Here's a graph I made of their assumptions about % change in estimated drug prices under single-payer. Under "high pay" assumptions Pharma revenue ~unchanged accounting for volume
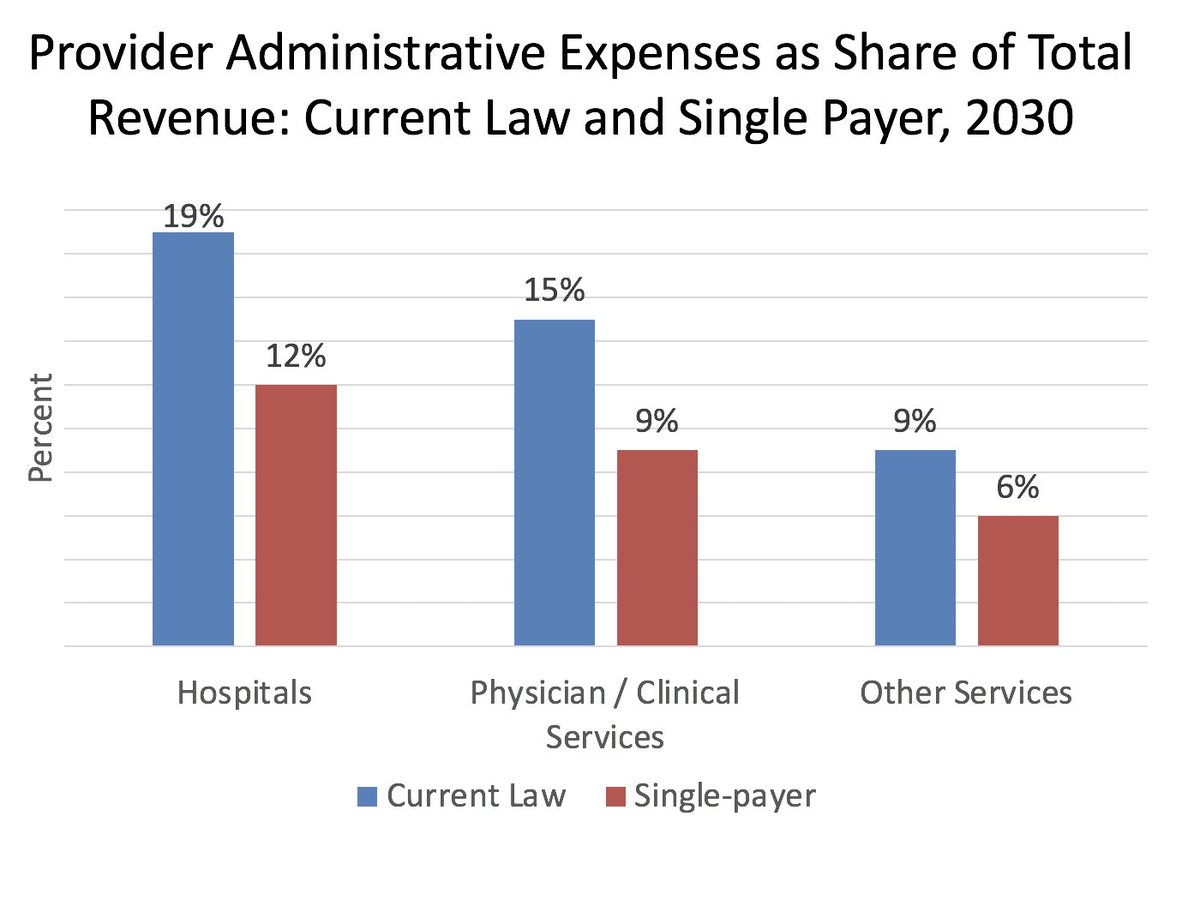
So, how do the numbers actually workout? Well, there's about $400 billion in payer-side administrative savings (Medicare Fee-for-Service, CBO assumes, has ~2% overhead, versus 12% among private insurers). There's also sharp reductions in provider-side administrative spending :
Relatively modest changes in overall hospital funding. Here's "low" cost-sharing, where inpatient and outpatient hospital care is free for everyone. Hospital revenue either rises or falls some depending on rate assumption, but remember small fall could be offset by admin savings
Revenue to physicians and clinicians is higher under every scenario of single-payer than it would be under the status quo, so nothing really here for physicians not to like. In addition, per CBO, they would have a ~50% reduction in time spent on administrative activities.
Apologies for variable quality of graphs and fonts. Also, realized I never linked to the report ! cbo.gov/publication/56…
(Also, to be clear, these are bar graphs I made to present CBO data).
I want to say a word about how utilization increases were modeled, an issue that I've done some research on in recent years with colleagues ... (A bit wonky from here) ...
The CBO report — unlike almost all other Medicare-for-All economic analyses in recent years — assumes supply constraints, e.g. finite doctors/hospital beds. Effectively, they contend that the total amount of healthcare utilized is effectively determined on the supply end...
Colleagues and I have argued similarly, a fact that helps explain why utilization increases after major coverage expansion in high-income nations have been mostly modest.
ajph.aphapublications.org/doi/10.2105/AJ…
annals.org/aim/article-ab…
.. link.springer.com/article/10.100…
ajph.aphapublications.org/doi/10.2105/AJ…
annals.org/aim/article-ab…
.. link.springer.com/article/10.100…
CBO rightly argues that supply constraints would constrain utilization increases under M4A. Consequently, they argue that even though everyone would be covered, healthcare would be mostly free, & overall use of care would rise, there'd also be an increase in "unmet demand"...
... manifested by increased provider "congestion," waiting times etc. But what this interpretation misses is the fact that much of the overall "demand" for healthcare is supplier-induced — and there is a great deal of wasteful over-provision in this country.
In other words, coverage expansions can lead to less useless care provided. See Glied & Hong, who found that when uninsurance rates for younger people rises, doctors respond by providing Medicare patients more care — but it's not useful healthcare!
pubmed.ncbi.nlm.nih.gov/29990674/
pubmed.ncbi.nlm.nih.gov/29990674/
So while the CBO is right to assume supply constraints (as few others have) & are also correct in assuming that this translates into less societywide utilization increase, this is likely mediated (at least largely) by less supplier-induced demand rather than more "unmet" demand.
This likely explains why concerns that the passage of Medicare in 1965 would lead to ERs and hospitals overflowing with patients never happened. Actually, there's no evidence I'm aware of that Medicare led to more unmet demand for those < 65 year or more provider congestion...
• • •
Missing some Tweet in this thread? You can try to
force a refresh