Interesting thanks, but can we really comment on misunderstandings relating to comparisons between vaccines while ignoring the elephant in the room:
Relative v Absolute risk reduction?
The vaccines are being pushed on the former while apparently nobody dare speak of the latter.
Relative v Absolute risk reduction?
The vaccines are being pushed on the former while apparently nobody dare speak of the latter.
https://twitter.com/brianrstill/status/1348293766063525890
Pre-2020, it would have been unarguable that consenting to a medical treatment should always be on the basis that the individual gives fully informed consent.
Fully informed involves describing risks v benefits.
I am not commenting in this thread on risks, only on benefits.
Fully informed involves describing risks v benefits.
I am not commenting in this thread on risks, only on benefits.
Effects on infection rates and transmissibility have not been demonstrated in these trials - only symptom reduction.
Hence any societal benefit via herd immunity is purely speculative, and ethically unjustifiable as the basis of coercion (which is unjustifiable anyway).
Hence any societal benefit via herd immunity is purely speculative, and ethically unjustifiable as the basis of coercion (which is unjustifiable anyway).
Hence it is the individual which matters, and for them, the benefit side of the ledger is not the relative risk reduction between the 2 groups in the trial.
It is the absolute risk reduction - what is the risk reduction that person is receiving?
From what risk TO what risk?
It is the absolute risk reduction - what is the risk reduction that person is receiving?
From what risk TO what risk?
The relative risk reduction is not relevant as it doesn't take account of background risk, ie in the absence of the procedure / treatment / vaccine, what is my risk anyway?
We could eliminate - that's right, we could achieve a 100% risk reduction - in death from appendicitis by removing everybody's appendix as infants.
Is this sensible?
No, because the risk of dying from appendicitis is incredibly low it's best just to treat it as it arises.
Is this sensible?
No, because the risk of dying from appendicitis is incredibly low it's best just to treat it as it arises.
A non-medical example:
The risk from air travel has been declining quite rapidly in recent decades.
(Since the pandemic it has been zero but that's another story....)
sciencedaily.com/releases/2020/…

The risk from air travel has been declining quite rapidly in recent decades.
(Since the pandemic it has been zero but that's another story....)
sciencedaily.com/releases/2020/…
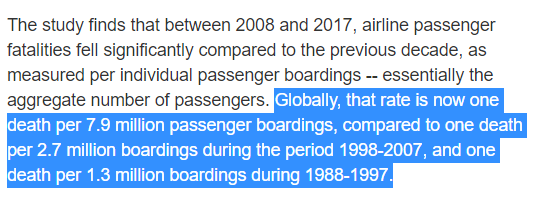
Imagine it was proposed that this could be reduced down even further, say to 1 in 80m.
1 in 7.9m to 1 in 80m is a 90% reduction is risk.
Great, let's do it!
OK - it means 4 hour check-ins, no hold baggage, and trebling ticket prices.
You never told me that!
1 in 7.9m to 1 in 80m is a 90% reduction is risk.
Great, let's do it!
OK - it means 4 hour check-ins, no hold baggage, and trebling ticket prices.
You never told me that!
Most people would say:
"the risk - at 1 in 7.9m - is so low anyway, it's something I can live with. We need / want to be able to travel at reasonable convenience and price.
Those measures just aren't worth it."
"the risk - at 1 in 7.9m - is so low anyway, it's something I can live with. We need / want to be able to travel at reasonable convenience and price.
Those measures just aren't worth it."
If someone said "but why wouldn't you want to make flying as safe as you could" you'd think them slightly deranged.
You'd explain that once a risk is so low, there are diminishing returns from trying to make it even lower.
After all, everything has risks, some unknown.
You'd explain that once a risk is so low, there are diminishing returns from trying to make it even lower.
After all, everything has risks, some unknown.
So, what are the absolute risk reductions for Covid19 vaccines from the trial data?
My sources are:
Pfizer:
Moderna:
AZ: fda.gov/media/144245/d…
fda.gov/media/144434/d…
assets.publishing.service.gov.uk/government/upl…
My sources are:
Pfizer:
Moderna:
AZ: fda.gov/media/144245/d…
fda.gov/media/144434/d…
assets.publishing.service.gov.uk/government/upl…
Pfizer vaccine:
Risk of Covid of any severity reduced from 0.74% to 0.04%
Risk of severe Covid reduced from 0.018% to 0.004
Risk of hospitalisation reduced from 0.004 to zero
>99.99% on placebo weren't hospitalised for Covid
Risk of Covid of any severity reduced from 0.74% to 0.04%
Risk of severe Covid reduced from 0.018% to 0.004
Risk of hospitalisation reduced from 0.004 to zero
>99.99% on placebo weren't hospitalised for Covid
Moderna:
Risk of Covid of any severity reduced from 0.64% to 0.04%
Risk of severe Covid reduced from 0.08% to 0.007%
Risk of hospitalisation reduced from 0.02% to zero
99.98% on placebo were not hospitalised for Covid
Risk of Covid of any severity reduced from 0.64% to 0.04%
Risk of severe Covid reduced from 0.08% to 0.007%
Risk of hospitalisation reduced from 0.02% to zero
99.98% on placebo were not hospitalised for Covid
AstraZeneca:
Risk of Covid of any severity reduced from 2.2% to 1%
Risk of severe Covid (WHO score ≥6) reduced from 0.02% to zero
Risk of hospitalisation reduced from 0.16% to 0.02%
99.84% on placebo were not hospitalised for Covid
Risk of Covid of any severity reduced from 2.2% to 1%
Risk of severe Covid (WHO score ≥6) reduced from 0.02% to zero
Risk of hospitalisation reduced from 0.16% to 0.02%
99.84% on placebo were not hospitalised for Covid
It should be stressed that not all the differences between active and placebo groups above reached "statistical significance".
But that's outside the scope of this thread.
I'm just reporting the raw data.
But that's outside the scope of this thread.
I'm just reporting the raw data.
Final point: these were deliberately conducted in countries with high prevalance to accelerate the trials.
Which is more significant:
- the reductions achieved between the groups
or
- how hard - under controlled conditions - it was to find any confirmed Covid, esp severe?
Which is more significant:
- the reductions achieved between the groups
or
- how hard - under controlled conditions - it was to find any confirmed Covid, esp severe?
Another way of lookimng at this is to determine the number needed to treat (MMT) to prevent a single case.
https://twitter.com/JavRoJav/status/1335027580181897217?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh