
Some days ago i had a pt with cirrhosis Child Pugh C admitted for AKI during my shift. Offending meds were withdrawn, IVC was seen at 0.9 cm and albumin infusion was started.
This common situation got my mind started: why is 🥚 so good for cirrhotic pts kidneys?
A brief 🧵:
👇🏽
This common situation got my mind started: why is 🥚 so good for cirrhotic pts kidneys?
A brief 🧵:
👇🏽

First, let's start by mentioning some of albumin's main properties:
🥚 67 kDa protein
🥚 Accounts for 75% of plasmatic oncotic pressure
🥚 Exclusively produced in the liver
🥚 Pleiotropic effects: 🚫 inflammatory, 🚫 oxidative & immunonodulatory
🥚 67 kDa protein
🥚 Accounts for 75% of plasmatic oncotic pressure
🥚 Exclusively produced in the liver
🥚 Pleiotropic effects: 🚫 inflammatory, 🚫 oxidative & immunonodulatory

Cirrhotic pts have ⬇️ 🥚 levels, but the one they do have gets dysfunctional:
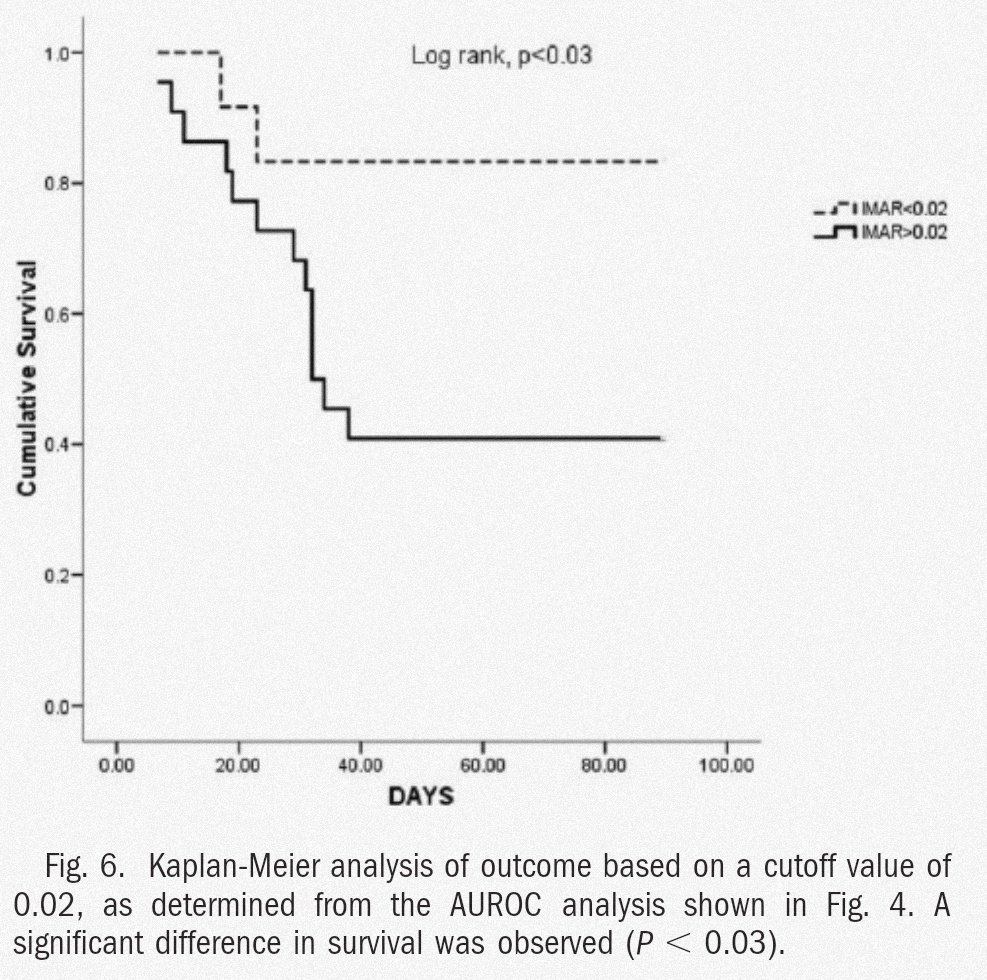
Proinflammatory and oxidative environment in decompensated cirrhotic pts oxidizes 🥚 and renders it uncapable of exerting its effects, ⬇️ "effective 🥚 concentration". This correlates w/ severity & ☠️!
Proinflammatory and oxidative environment in decompensated cirrhotic pts oxidizes 🥚 and renders it uncapable of exerting its effects, ⬇️ "effective 🥚 concentration". This correlates w/ severity & ☠️!


Apart from 🥚 dysfunction, cirrhotic pts have 🩸dynamic alterations that make them prone to AKI:
❤️ ⬆️ portal pressure 2/2 structural (fibrosis, nodule formation, thrombosis) & dynamic (⭐ cells responsive to vasoactive agents)
❤️ ⬇️ SVR & EAV
❤️ ⬆️ CO
❤️ ⬆️ RAAS, ADH & SNS
❤️ ⬆️ portal pressure 2/2 structural (fibrosis, nodule formation, thrombosis) & dynamic (⭐ cells responsive to vasoactive agents)
❤️ ⬇️ SVR & EAV
❤️ ⬆️ CO
❤️ ⬆️ RAAS, ADH & SNS
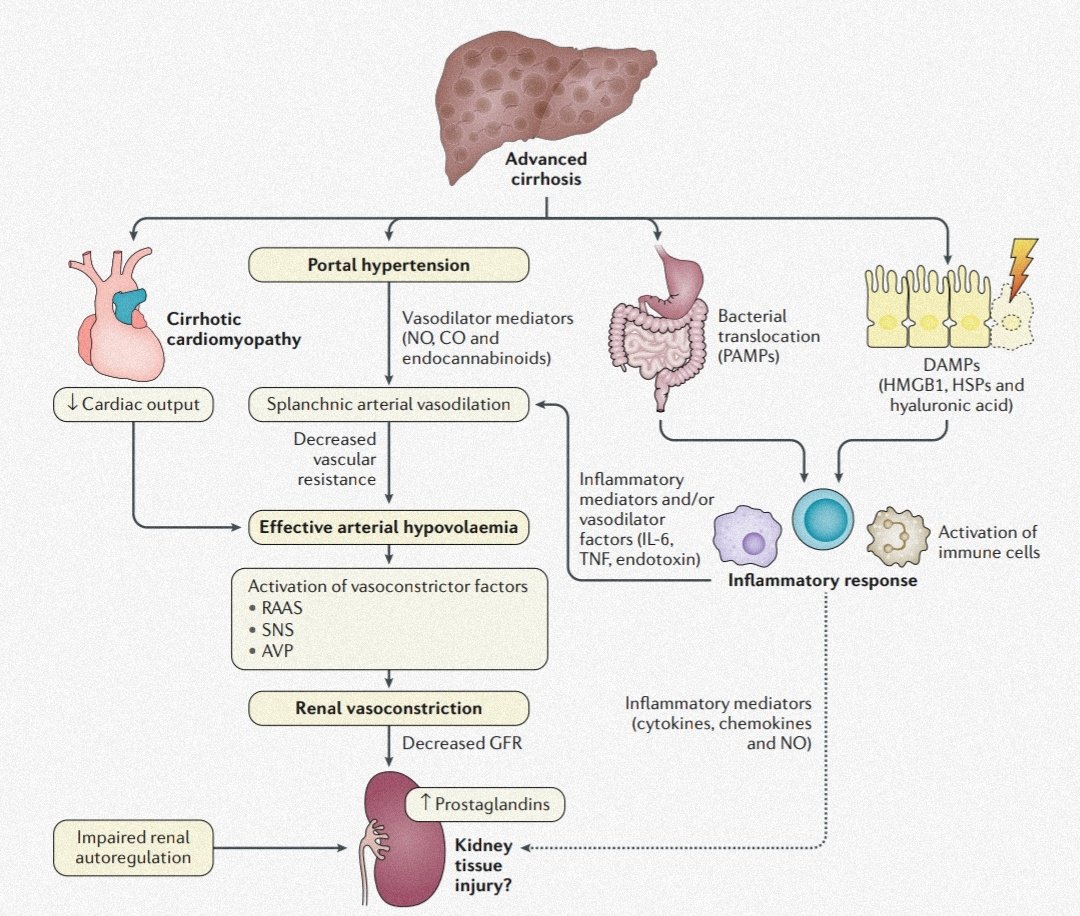
Portal ⬆️tension causes splanchnic vasodilation, but... what are the mediators involved here?
Splanchnic vasodilation is thought to be caused by ⬆️ in NO, CO & endocannabinoids. This ➡️ to ⬇️ SVR & EAV, compensated by an ⬆️ in CO 1️⃣ and 2️⃣ by ⬆️ RAAS, ADH & SNS activity.
Other contributors to decompensation are inflammation, cirrhotic ❤️myopathy & ⬇️ renal prostaglandin
Other contributors to decompensation are inflammation, cirrhotic ❤️myopathy & ⬇️ renal prostaglandin

So where does albumin fit in this puzzle of deranged physiology? Well, it fits everywhere! For example, in pts treated with paracentesis, 🥚 administration ⬇️ readmission probability, hyponatremia and renal impairment:



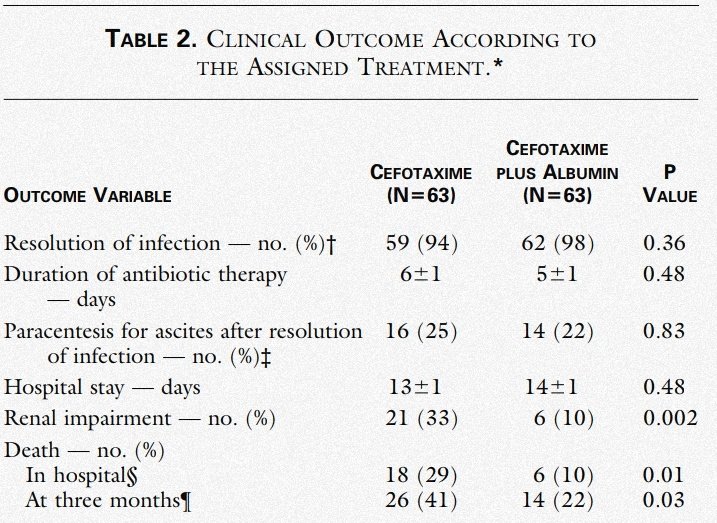
Likewise, in pts developing SBP, 🥚 administration ⬇️ renal impairment & ☠️, and also correlated w/ ⬇️ plasmatic renin activity:


AKI in cirrhotic pts requires special consideration because of the broad differential and the risk of progression to HRS. For that matter, I find this algorythm by @VelezNephHepato et al. a great tool:

Along the same line of thought, not every AKI in cirrhotic pts is going to be fluid responsive, and for that matter, this clinical case and analysis by my good friend @ArgaizR settles the question nicely!
criticalcarenow.com/2020/10/04/alb…
criticalcarenow.com/2020/10/04/alb…
But what if our pt does progress to the feared HRS? Well, 🥚 has applications there too! In this study, addition of albumin to terlipressin in HRS mgmt ⬇️ sCr, ⬆️ pb of survival @ 90 days & ⬆️ rates of complete response (77% in 🥚+ terli group vs 25% in terli alone)




Wrapping up this brief rant on 🥚 magical properties:
🥚 Has 🚫inflammatory, 🚫oxidative & immunonodulatory effects
🥚 dysfunctional as severity of cirrhosis⬆️
🥚 Useful in LVP, SBP, AKI, HRS & more!
🥚 Not every AKI responds to 💧, 👀JVP (as per @AndreMansoor) & POCUS useful
🥚 Has 🚫inflammatory, 🚫oxidative & immunonodulatory effects
🥚 dysfunctional as severity of cirrhosis⬆️
🥚 Useful in LVP, SBP, AKI, HRS & more!
🥚 Not every AKI responds to 💧, 👀JVP (as per @AndreMansoor) & POCUS useful
Hope you enjoyed this 🧵!
Sources (PMID or DOI):
3360270
19642174
31723234
30213943
12297842
10432325
32102926
10.1016/j.mam.2007.09.010
Sources (PMID or DOI):
3360270
19642174
31723234
30213943
12297842
10432325
32102926
10.1016/j.mam.2007.09.010
@sargsyanz @ebtapper @WrayCharles @thecurbsiders @DxRxEdu @CPSolvers @AvrahamCooperMD @CuriousClinPod @AdamRodmanMD @medpedshosp @DoctorWatto @AllisonRBond
• • •
Missing some Tweet in this thread? You can try to
force a refresh


