
1/5 An interesting illustrative case of the day. 62-year-old man with mid ventricular HCM associated with a large apical aneurysm #EchoFirst @AAH_StLukesCV
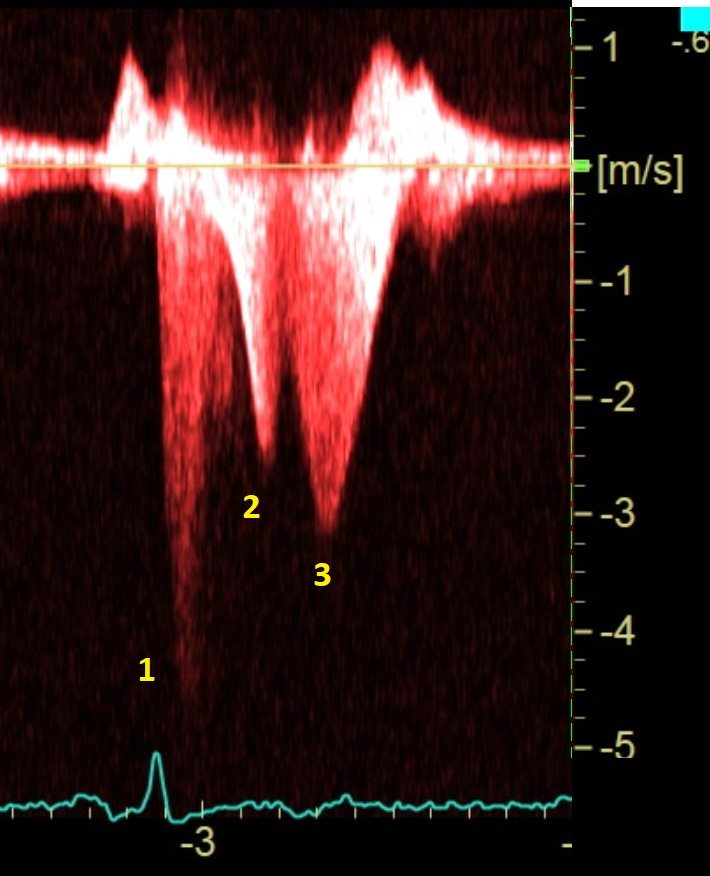
2/5 CW Doppler trace shows triphasic flow:
1. MR
2. Mid ventricular obstruction
3. Outflow from the apex towards mid LV cavity during IVRT.
1. MR
2. Mid ventricular obstruction
3. Outflow from the apex towards mid LV cavity during IVRT.
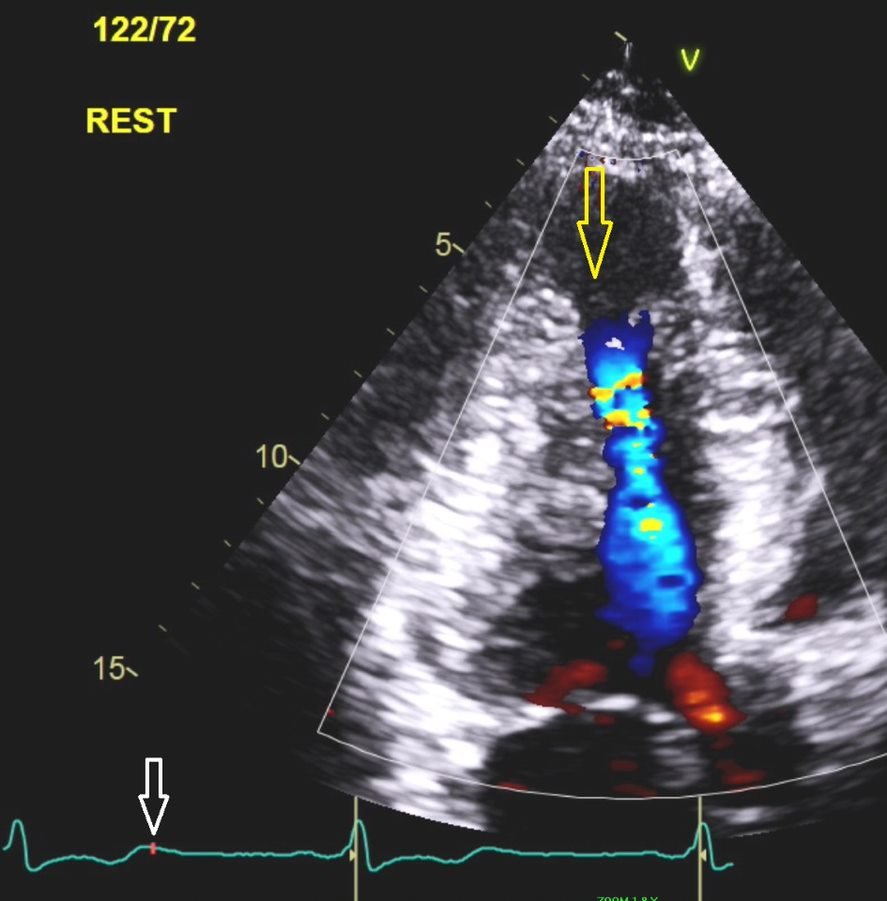
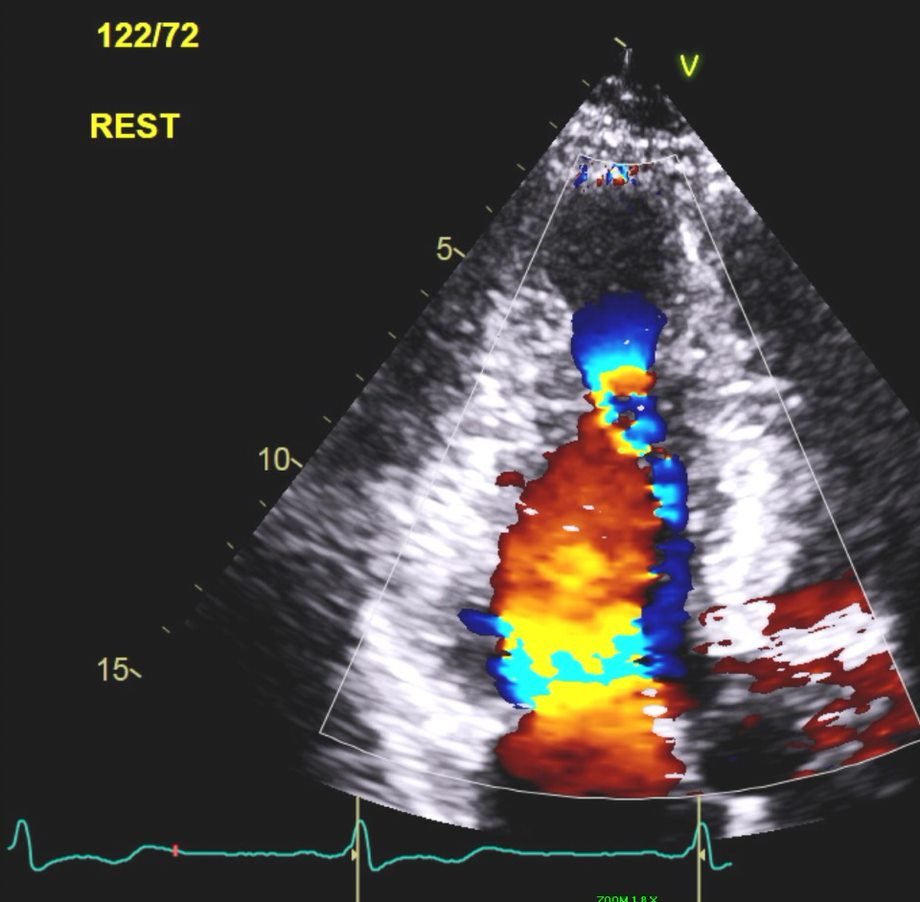
3/5 This characteristic flow pattern is also visualized on 2D color flow (still images below).
4/5 Left: Flow during IVRT (blue jet/arrow).
Right: Flow after MV opening (red jet). Note the two flows "colliding" in the mid ventricle.
Right: Flow after MV opening (red jet). Note the two flows "colliding" in the mid ventricle.
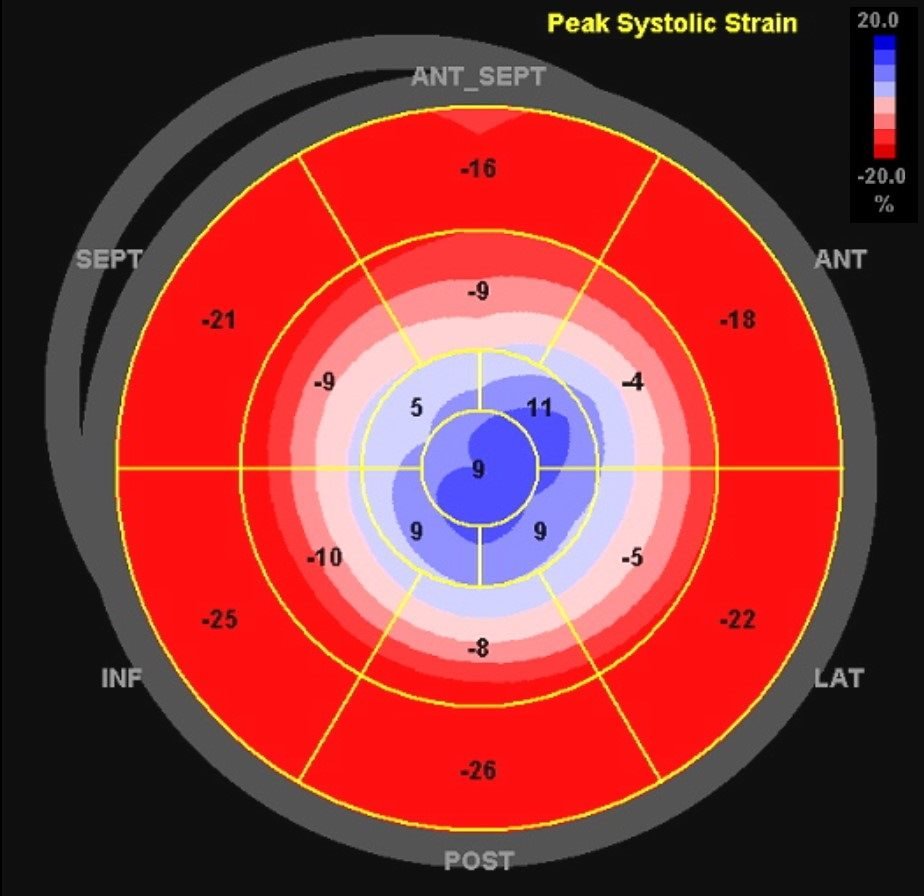
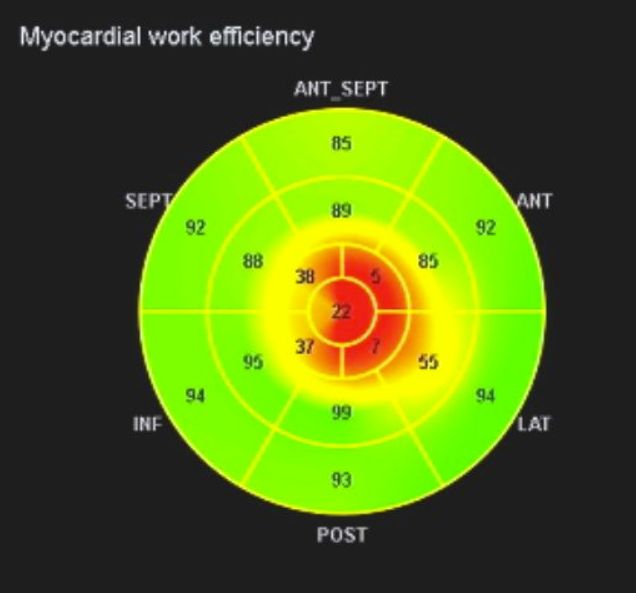
5/5 Bullseye strain is typical of apical aneurysm with dyskinesis shown in deep blue. Global work efficiency is markedly decreased at 66% due to apical dyskinesis.
@JaeKOh2 @BijoyKhandheria @JACCJournals @ASE360 @ESC_Journals @mahali87 @SteveOmmen @jeffreygeske @renujain19 @Lakshmi14524052 @PatrycjaGalazka @KyleWKlarich @fuadfehmi @AllaqabanSuhail @AsadGhafoor79 @HFSA
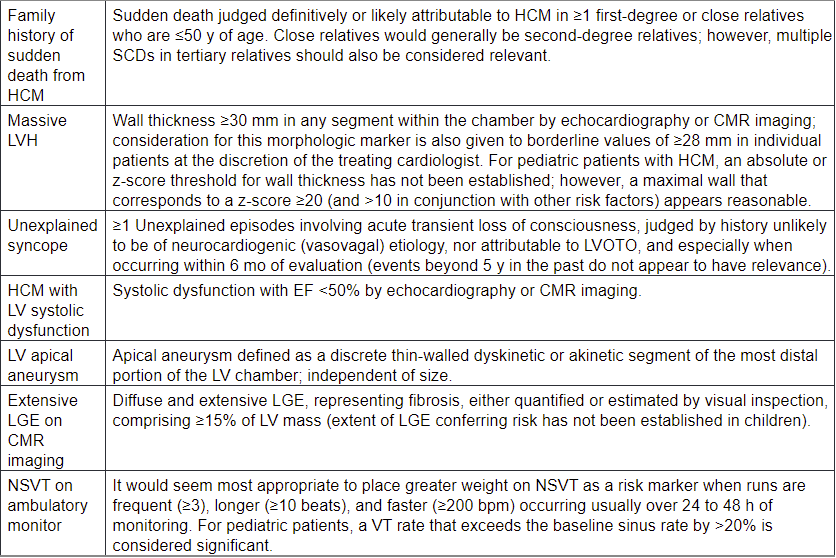
#echofirst I appreciate all the comments and questions related to this tweet. This HCM phenotype is now included in the latest ACC/AHA guidelines as a high risk marker SCD, and indication for ICD placement, which was performed in this patient.
ahajournals.org/doi/10.1161/CI…
ahajournals.org/doi/10.1161/CI…

Patient was reluctant to start warfarin, instead given NOAC. While on NOAC developed an apical thrombus that was complicated by splenic embolic infarct. Currently on warfarin.
Distinction from diverticulum is the fibrotic wall of this true aneurysm on #whyCMR
• • •
Missing some Tweet in this thread? You can try to
force a refresh





