
Step-by-step tweetorial on percutaneous post-infarct VSD closure. Late presenting inferior MI.
Cardiac CT can be very helpful in planning the approach and in noting nearby structures. Here, the defect is quite basal - semilunar valves can disrupted.
1- GA and TEE guidance. Note proximity of the defect to the tricuspid valve.
2- Bifemoral arterial and venous access was obtained. LV gram performed in LAO CRA. This will help guide crossing of the defect (can be challenging).
3- Exchange pigtail for a catheter (we used AR1) and cross the defect with an exchange length wire (we used angled glide). Send the glide to the PA where it will be snared. 
4- Snare the exchange glide from the PA (we used a 25 mm gooseneck/MP guide) then externalize. Via the venous limb, insert a 100cm glide catheter into the Ao. Through this, advance a stiff wire (we used exchange Rosen). Snare the Rosen from the Ao and externalize. Rail ready.


5- Through-out all this, TEE will help with guidance and to ensure wire not entangled in subvalvular apparatus.
6- Advance delivery sheath across defect (usually via venous limb) as far as it can go. Can attempt to deliver an 0.018 wire to secure access across defect. Deploy device (see below for device selection).
7- LV gram and TEE revealed interaction of RV disk with the tricuspid valve despite multiple attempts to redeploy the the device. Note the line below on RV side is septal leaflet of TV.
8- TEE revealing interaction of RV disk with TV.
9- We changed strategies and deployed the device via the arterial side. Delivery system (Amplatzer) was not be long enough 10Fr 80cm via Ao side, hence, we used a 90 cm 8Fr shuttle sheath. Required acrobatics to get device into the sheath.

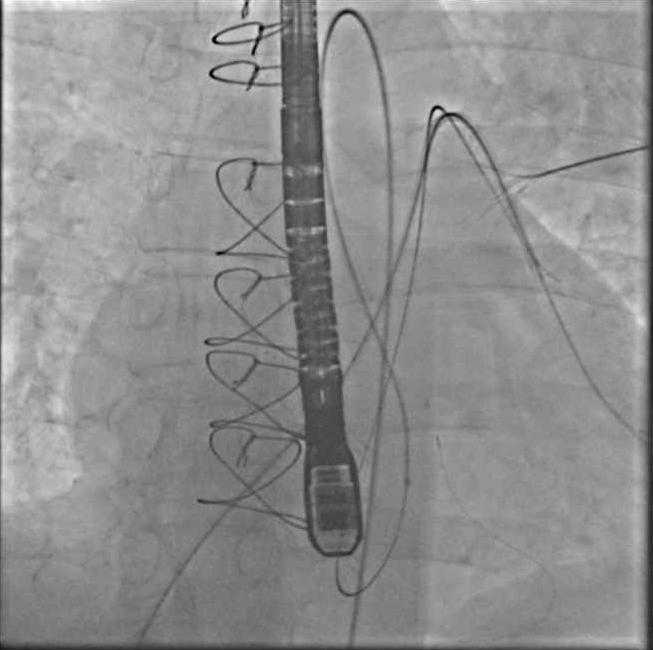
10- Device deployed successfully without interacting with valvular structures. Qp:Qs dropped from 2.3 to 1.2. SBP acutely increased 40-50 points. Note: Usually takes time for a good seal to form.
11- Final TEE image. Device stable.
Device selection: Unlike muscular VSD's, post-infarct VSDs are usually serpiginous, which affects device selection. We used a 30 mm Amplatzer Cribriform Septal Occluder (designed for fenestrated ASD's). Case series below showed that device selection depends on the anatomy.


Final note: For rare and complex structural/interventional procedures, it is always good to keep step-by-step notes for future reference. #ACCFIT

Any other tips/tricks re post-infarct VSD closure? @BrighamFellows @Almanfi_Cardio @didier_tchetche @AlkashkariWail @Tod_Maddux @AshvinPande @AGoldsweig @CathElectroSurg @bkolskk @ekgpdx @spiritus_bah @duanepinto @jtsaxon @akcmahi @PaulMahoneyMD @BGalperMD @HarshGMD @PedroMDMSc
Thank you all for the feedback and tips. Big shoutout to @PinakShahMD @TsuyoshiKaneko1 for the amazing structural training at the BWH cath lab.
• • •
Missing some Tweet in this thread? You can try to
force a refresh









