Parenchymal changes caused by liver hemodynamic alterations (pseudotumor).
Small areas of liver tissue are known to be supplied by a "third inflow" venous system separate from the usual dual blood supply of the portal vein and hepatic artery.
Small areas of liver tissue are known to be supplied by a "third inflow" venous system separate from the usual dual blood supply of the portal vein and hepatic artery.

This is a normal variant and it is composed of aberrant veins or parts of normal veins that directly enter the liver independently of the portal venous system; such veins communicate with intrahepatic portal branches to various degrees.

Areas of focal fatty sparing and focal steatosis may develop due to altered hepatic blood flow associated with these vessels. The concentrations of hormones (eg. insulin), and nutrients (eg. dietary fat), in the third inflow, could be different from those in the portal blood.



These differences could contribute to the heterogeneous deposition of fat. The reason why similar variations in blood supply cause focal fatty infiltration in some patients and focal spared area in others is still unknown.
Pearl: Third inflow can also play an important role in the blood supply of the liver in the setting of portal vein thrombosis.
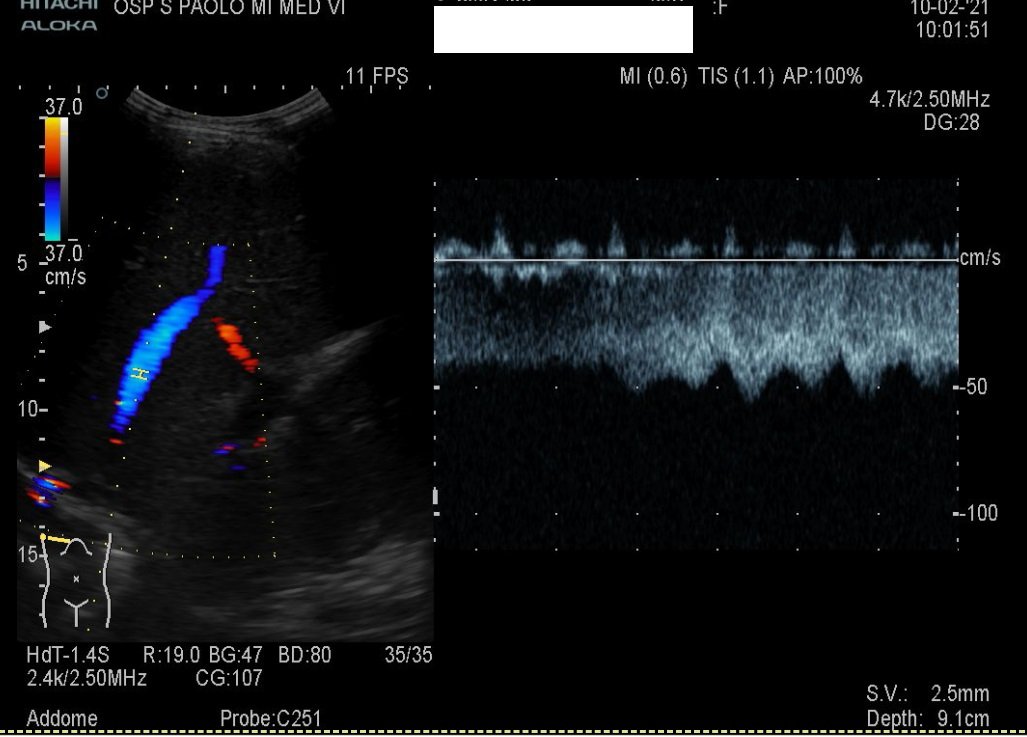
Below an example in a 53y man with large areas of focal steatosis results of massive portal thrombosis (Antiphospholipid syndrome).
Below an example in a 53y man with large areas of focal steatosis results of massive portal thrombosis (Antiphospholipid syndrome).


References:
> pubs.rsna.org/doi/full/10.11…
>openaccessjournals.com/articles/radio…
@hepocus @NephroP @IMPOCUSFocus @HunPocus @POCUS_spain @pocusfoamed @POCUS_Society @OSUultrasound @AafpMig @daniel_opazo @POCUSAcademy @Pocus101 @ultrasoundcases @trigeminy_henry
> pubs.rsna.org/doi/full/10.11…
>openaccessjournals.com/articles/radio…
@hepocus @NephroP @IMPOCUSFocus @HunPocus @POCUS_spain @pocusfoamed @POCUS_Society @OSUultrasound @AafpMig @daniel_opazo @POCUSAcademy @Pocus101 @ultrasoundcases @trigeminy_henry
• • •
Missing some Tweet in this thread? You can try to
force a refresh