NYC's COVID data has been screwed up lately so here's what the state's data shows for NYC:
Cases (7-day average)
Current: 3921
1 week ago: 3854
2 weeks ago: 3797
3 weeks ago: 3999
Positive test rate (7-day avg)
Current: 4.3%
1 week ago: 4.3%
2 weeks ago: 3.9%
3 weeks ago: 4.2%
Cases (7-day average)
Current: 3921
1 week ago: 3854
2 weeks ago: 3797
3 weeks ago: 3999
Positive test rate (7-day avg)
Current: 4.3%
1 week ago: 4.3%
2 weeks ago: 3.9%
3 weeks ago: 4.2%
On the one hand, I'm pretty sure that sites showing a decline in NYC (the NYT shows this, for example) are wrong. They're filling in missing city data with state data for the city. But that state data isn't apples-to-apples; it doesn't include probably cases, for instance.
On the other hand, I'm seeing a lot of loose talk about a "spike" in NYC when, no, that isn't really justified either. For better or worse, the numbers have settled into a plateau, which is also the case throughout the Northeast. beta.healthdata.gov/Health/COVID-1… 
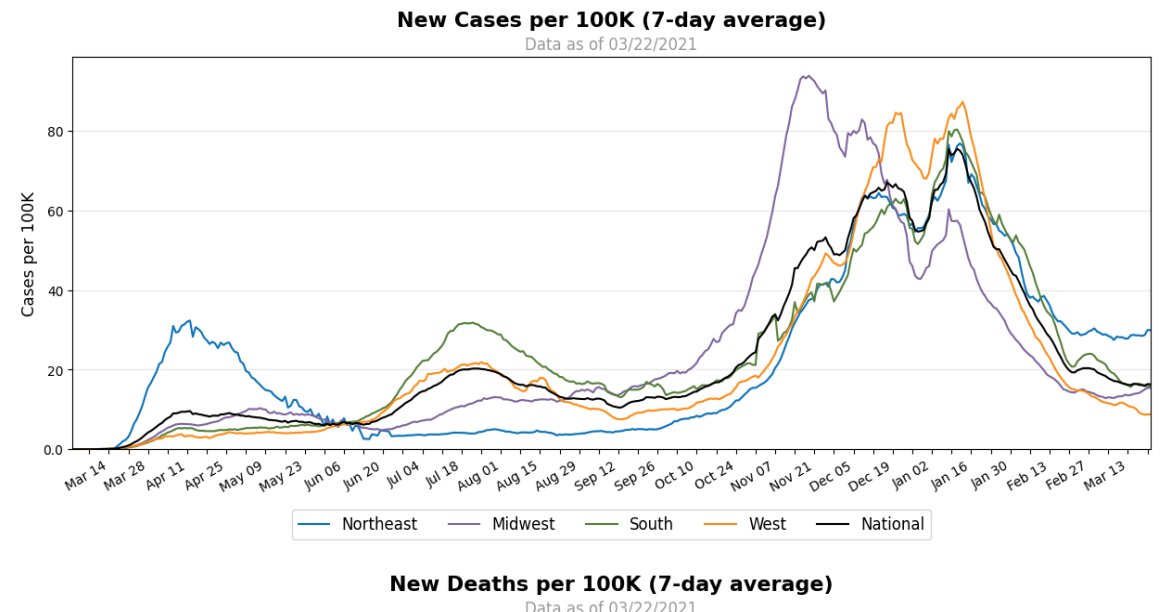
NYC/NYS have reasonably high per-capita rates of COVID cases, but you need to adjust for testing volumes when comparing across states. Per capita, NYS is doing ~2.5 more tests per capita than the US overall, so we're capturing more of our infections than most states do.
Boroughwise, here is the current 7-day average case counts as compared to 3 weeks ago:
Borough: Now / 3 weeks ago
Queens: 1180 / 1093
Brooklyn: 1184 / 1228
Bronx: 645 / 794
Manhattan: 612 / 629
S.I.: 301 / 255
Borough: Now / 3 weeks ago
Queens: 1180 / 1093
Brooklyn: 1184 / 1228
Bronx: 645 / 794
Manhattan: 612 / 629
S.I.: 301 / 255
Update: NYC finally updated its COVID data and it agrees with the state, more or less. Clear signs of a plateau in cases and the positive test %.
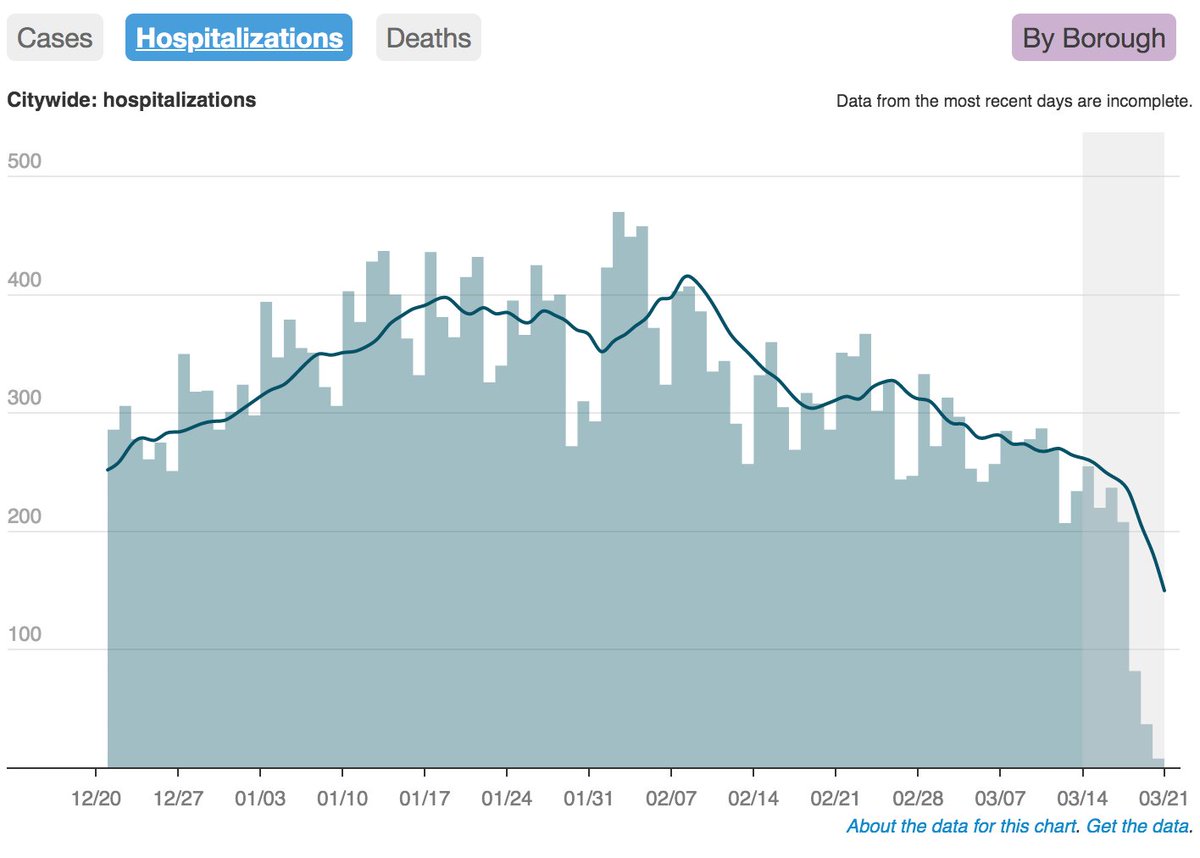
Hospitalizations still declining (though ignore the grey part of the chart, which has incomplete reporting). www1.nyc.gov/site/doh/covid…
Hospitalizations still declining (though ignore the grey part of the chart, which has incomplete reporting). www1.nyc.gov/site/doh/covid…

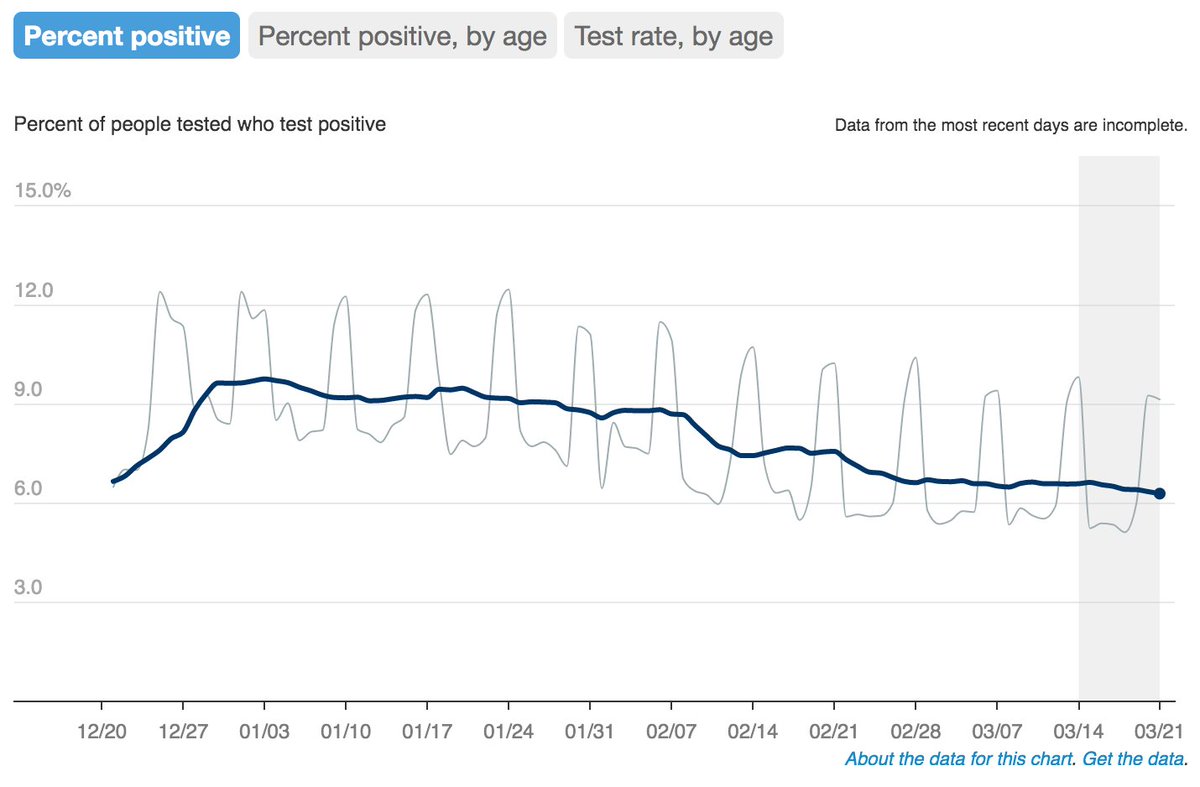
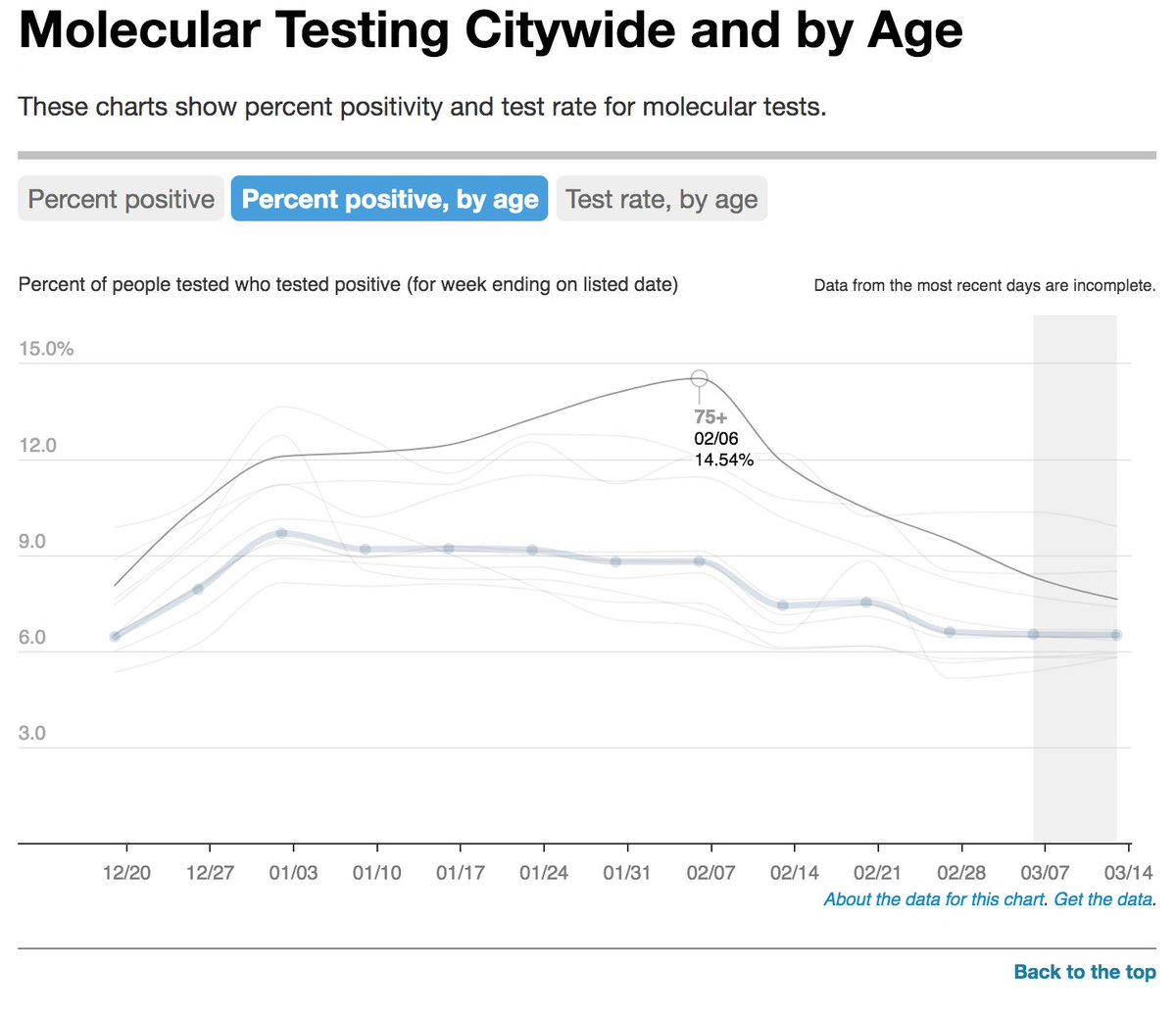
Bonus tweet: Nice plunge in positive test rates for people aged 75+ in NYC, who were the first to be vaccinated.
• • •
Missing some Tweet in this thread? You can try to
force a refresh