
Carney triad vs. Carney dyad 🧬 #endotips (thread👇)
A diagnosis of Carney triad requires co-existing paraganglioma (PGL), pulmonary chondroma, and gastrointestinal stromal tumor (GIST) with either a germline pathogenic variant in SDHx or SDHC locus-specific hypermethylation
A diagnosis of Carney triad requires co-existing paraganglioma (PGL), pulmonary chondroma, and gastrointestinal stromal tumor (GIST) with either a germline pathogenic variant in SDHx or SDHC locus-specific hypermethylation

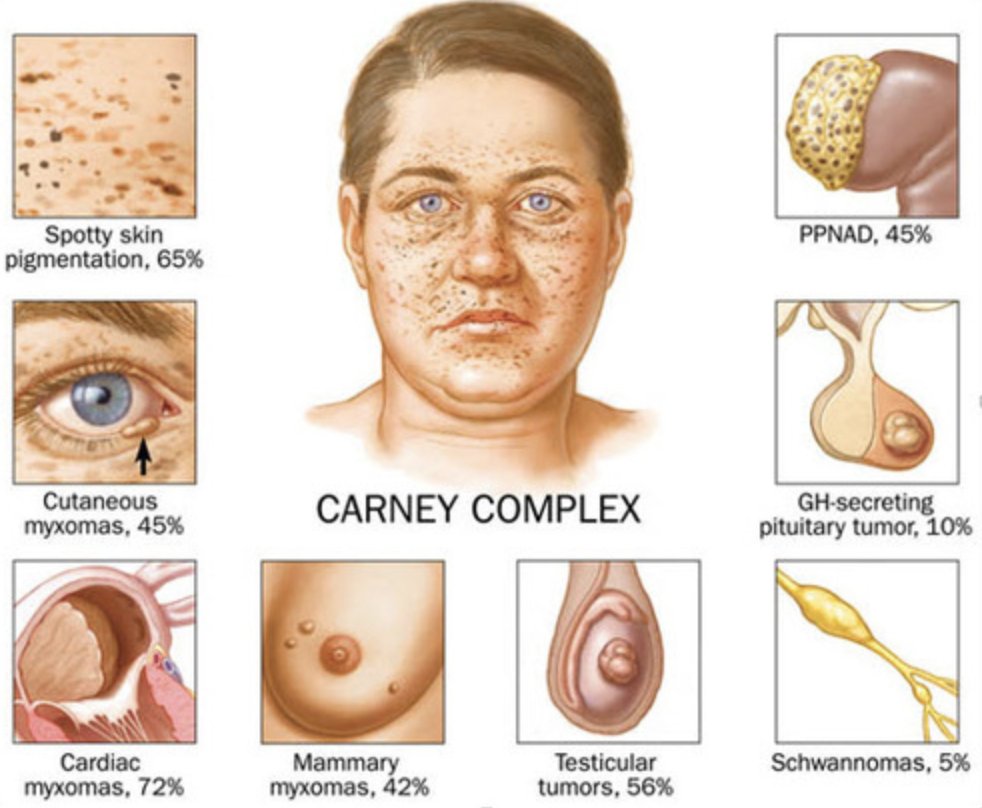
In contrast, Carney dyad is the association of PGL and GIST with a germline pathogenic variant in SDHx. Don't confuse them with Carney complex, an autosomal dominant lentiginosis syndrome with myxomas, endocrine tumors or overactivity, and schwannomas👇
Carney-Stratakis syndrome is another name for Carney diad (discovered by two giants in the field, Dr Aidan Carney from @MayoClinic and Dr Constantine Stratakis from @NIH)

More info here in our new publication @EDMCaseReports edm.bioscientifica.com/view/journals/… @Crystal_k4md @rachel_wurth @ConstantineStr7 @NIH @NICHD_NIH
Carney triad has a fourth component, adrenal cortical adenoma (either micro or macro) or hyperplasia + subclinical hypercortisolism: the only known disease with predisposition to BOTH adrenocortical and adrenomedullary (pheochromocytoma) lesions
journals.lww.com/ajsp/Fulltext/…
journals.lww.com/ajsp/Fulltext/…

• • •
Missing some Tweet in this thread? You can try to
force a refresh







