
1/ To delay 2nd doses of the Pfizer and Moderna COVID vaccines (like the UK, Germany, & Canada)?
usatoday.com/story/opinion/…
Or not to delay?
thinkglobalhealth.org/article/dont-b…
That is the question.
usatoday.com/story/opinion/…
Or not to delay?
thinkglobalhealth.org/article/dont-b…
That is the question.
2/ Where there is this much disagreement among experts (BTW, some arguing for delaying 2nd doses are some of my favorite people!) and the stakes are this high, not only for individuals but also for populations, the only way to resolve the question is through empirical study.
3/ Agreed, though I think deaths will be blunted by our having vaccinated many of the highest risk (i.e. residents of long-term care facilities and people 65 and older). 

4/ We have shown a reduction in the risk of infection (individual-level data) but not yet a reduction in transmission (population-level study). The PreventCOVIDU.org will help address the question of whether the Moderna vaccine reduces transmission.
wsj.com/articles/covid…
wsj.com/articles/covid…

5/ The problems at the Emergent BioSolutions manufacturing plant are inexcusable. This cannot be allowed to happen again.
nytimes.com/2021/04/07/us/…
nytimes.com/2021/04/07/us/…
6/ We don't know that vaccination curbed the surge in the UK. It could have been the result of strict months-long lockdowns. They’re only now just starting to reopen: bbc.com/news/explainer…
The real test will be whether there's a rebound in cases after the UK reopens.
The real test will be whether there's a rebound in cases after the UK reopens.

7/ Agreed. And you may have even more robust and durable immune responses if you delay the 2nd dose by 12 weeks, but we don't know that. That would need to be studied.
8/ What worries me and many others is not what happens after the 2nd dose, but rather what happens between the first and second doses. Are you creating a window when you have intermediate levels of immunity creating immune pressure on the virus?
9/ Immunity isn’t binary.
It’s on a continuum.
It’s not immune versus not immune.
It’s immune against some variants and not immune or partially against others.
It’s on a continuum.
It’s not immune versus not immune.
It’s immune against some variants and not immune or partially against others.

10/ We don’t know the effectiveness of one dose of mRNA vaccine beyond a few weeks.
See data from Scotland: ed.ac.uk/files/atoms/fi…
Look at Table 2 for Pfizer vaccine.
See data from Scotland: ed.ac.uk/files/atoms/fi…
Look at Table 2 for Pfizer vaccine.
11/ Vaccine efficacy (VE) for HOSPITALIZATION peaks at 85% at 28-34 days after 1st dose. However, 35-41 days after, VE drops to 68%, and 42+ days after, VE drops to 64%. This is VE as measured by hospitalization, which means that the VE against INFECTION is going to be lower.

12/ How much viral replication will you have in this setting? How much transmission? We don’t know.
But this is the very window between 1st and 2nd doses that we're worried about.
But this is the very window between 1st and 2nd doses that we're worried about.
13/ I don't buy this equity argument.
Given the risks involved, it would be like saying: I have two patients with AIDS and CD4+ T-cell counts of 50.
I have only enough guaranteed ongoing supply of rilpivirine and tenofovir/emtricitabine for one person.
Given the risks involved, it would be like saying: I have two patients with AIDS and CD4+ T-cell counts of 50.
I have only enough guaranteed ongoing supply of rilpivirine and tenofovir/emtricitabine for one person.
14/ Do I give Edurant and Descovy to one patient?
Or Edurant to one patient and Descovy to the other?
Or Edurant to one patient and Descovy to the other?
15/ If you give Edurant + Descovy to one patient, you could save that patient's life.
If you give Edurant to one patient and Descovy to the other, both patients end up with drug-resistant HIV virus and eventually die. Is that more equitable?
If you give Edurant to one patient and Descovy to the other, both patients end up with drug-resistant HIV virus and eventually die. Is that more equitable?
16/ Equity in vaccine distribution would mean allocating our vaccine supply according to risk--i.e. the populations who've had the most infections, hospitalizations, and deaths from COVID--not according to population size... or high-income the country.
17/ We haven't shown that COVID vaccination prevents transmission yet (population outcome). We've only shown that vaccination reduces the risk of infection (individual outcome). It stands to reason that reducing infection will reduce transmission, but we don't know by how much.
18/ This is mostly true. There is speculation about the risks of delaying 2nd doses AND about the risks of continuing to give both doses on time. BOTH are SPECULATION. The only way to settle the question is to study it empirically.
19/ There are just too many variables at play to say what delaying 2nd doses will mean with respect to selection for vaccine-escape variants. I don’t think we can reason our way to an answer here. I’m not sure that even modeling will get us there.
20/ However, we already do have evidence of the risks of delaying second doses:
nature.com/articles/s4159…
nature.com/articles/s4159…
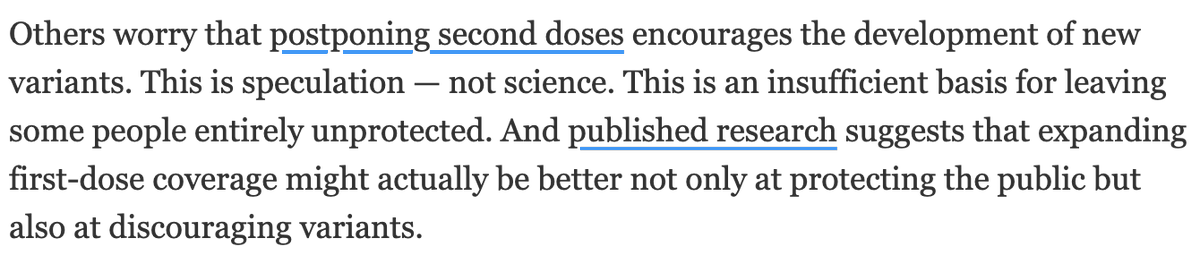
21/ See Fig 4a:
When was neutralization detectable after getting with Pfizer vaccine?
D614G (early strain): 2 weeks after 1st dose
B.1.1.7: 3 weeks after 1st dose (but less well)
B.1.351: 4 weeks after 1st dose = 1 week after 2nd dose (lower than for D614G or B.1.1.7)
When was neutralization detectable after getting with Pfizer vaccine?
D614G (early strain): 2 weeks after 1st dose
B.1.1.7: 3 weeks after 1st dose (but less well)
B.1.351: 4 weeks after 1st dose = 1 week after 2nd dose (lower than for D614G or B.1.1.7)
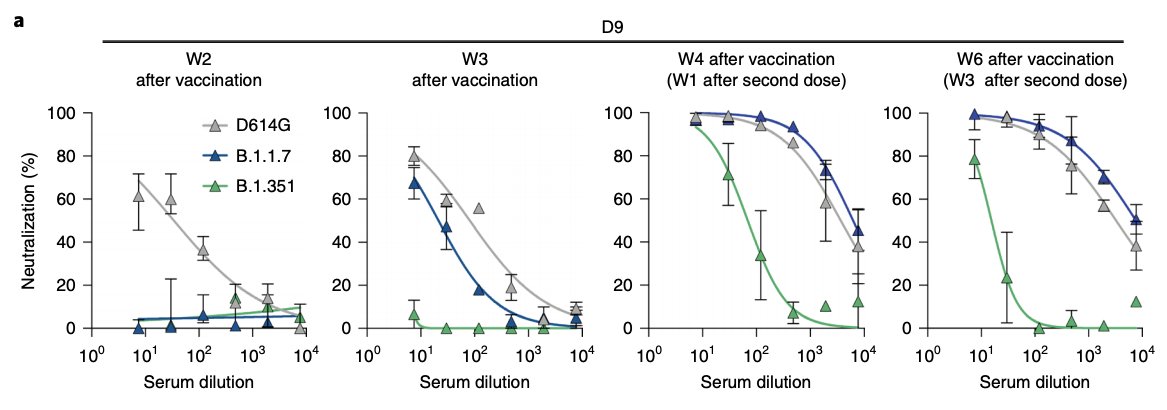
22/ See Fig 4d:
3 weeks after 1st dose, 63% neutralizers vs D614G and 38% neutralizers vs B.1.1.7.
The 2nd dose of Pfizer vaccine is important for boosting levels of neutralizing antibodies and to widen coverage of variants.
3 weeks after 1st dose, 63% neutralizers vs D614G and 38% neutralizers vs B.1.1.7.
The 2nd dose of Pfizer vaccine is important for boosting levels of neutralizing antibodies and to widen coverage of variants.
23/ The last thing we need is to be selecting for E484K-carrying B.1.1.7 variants with a weeks-long window of intermediate immune responses.
24/ researchsquare.com/article/rs-226…
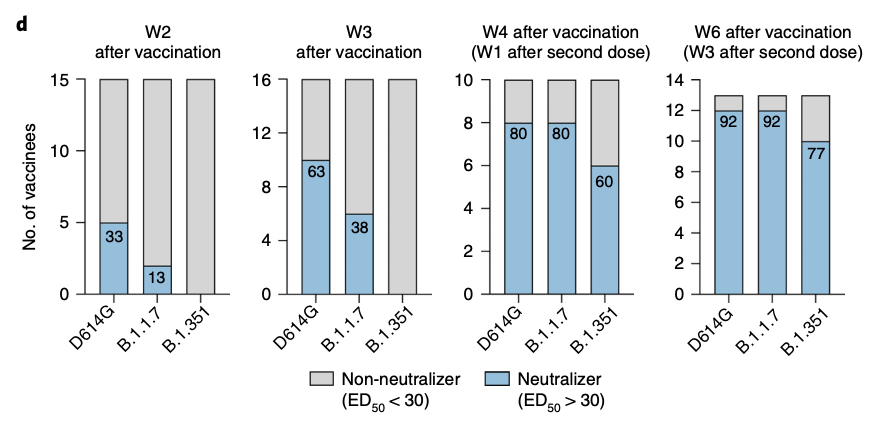
See Fig 2D
Black: neutralizing antibody responses in people after natural infection
Blue: neutralizing antibody responses in people who’ve had 1 dose of Pfizer vaccine
Pink: neutralizing antibody responses in people who’ve had 2 doses of Pfizer vaccine
See Fig 2D
Black: neutralizing antibody responses in people after natural infection
Blue: neutralizing antibody responses in people who’ve had 1 dose of Pfizer vaccine
Pink: neutralizing antibody responses in people who’ve had 2 doses of Pfizer vaccine
25/ One dose is good enough against the original strains of the virus (B VIC01).
But you really need two doses of vaccine against the B.1.1.7 and B.1.351 variants.
But you really need two doses of vaccine against the B.1.1.7 and B.1.351 variants.
26/ sciencedirect.com/science/articl…
See Fig 4:
Persons who received only one dose of Pfizer or Moderna vaccine had lower and in some cases undetectable neutralization of the B.1.1.7, P1 & other variants of concern even though they had activity against the original strains of SARS-CoV-2.
See Fig 4:
Persons who received only one dose of Pfizer or Moderna vaccine had lower and in some cases undetectable neutralization of the B.1.1.7, P1 & other variants of concern even though they had activity against the original strains of SARS-CoV-2.

27/ Among those who received only one dose of Pfizer or Moderna vaccine, none had neutralizing activity against B.1.351 EXCEPT for those who had previously been infected or had a significant exposure.
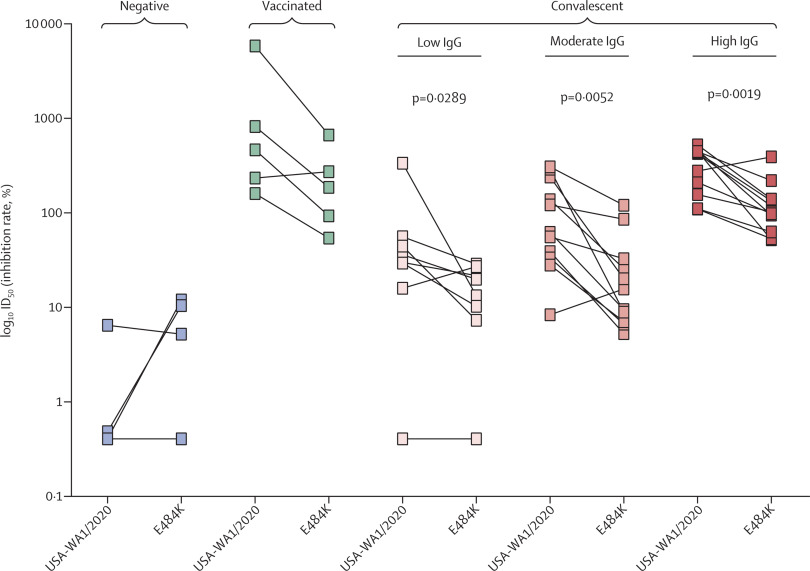
28/ thelancet.com/journals/lanmi…
Serum taken from people who received TWO doses of Pfizer vaccine had lower neutralizing efficiency against SARS-CoV-2 virus with the E484K EEK immune-evasion mutation versus against the original strains of the virus.
Serum taken from people who received TWO doses of Pfizer vaccine had lower neutralizing efficiency against SARS-CoV-2 virus with the E484K EEK immune-evasion mutation versus against the original strains of the virus.
29/ Vaccines should induce the highest neutralizing antibody titers possible to maximize protection against SARS-CoV-2 mutation and evolution to evade vaccine-induced immune responses.
30/ In summary, we have evidence that neutralizing antibody levels after 1st dose of Pfizer and Moderna vaccines are NOT very effective against B.1.1.7 (now the dominant variant in the U.S.) or the B.1.351 variant.
31/ Moreover, we know that 2nd doses of vaccine are necessary to provide a significant boost to neutralizing antibody levels.
Here’s the data on the Pfizer vaccine:
Here’s the data on the Pfizer vaccine:
https://twitter.com/celinegounder/status/1358443839640502272?s=20
32/ Studies have shown that 2nd doses of Moderna vaccine boost antibody levels significantly:
https://twitter.com/celinegounder/status/1358444252875915264?s=20
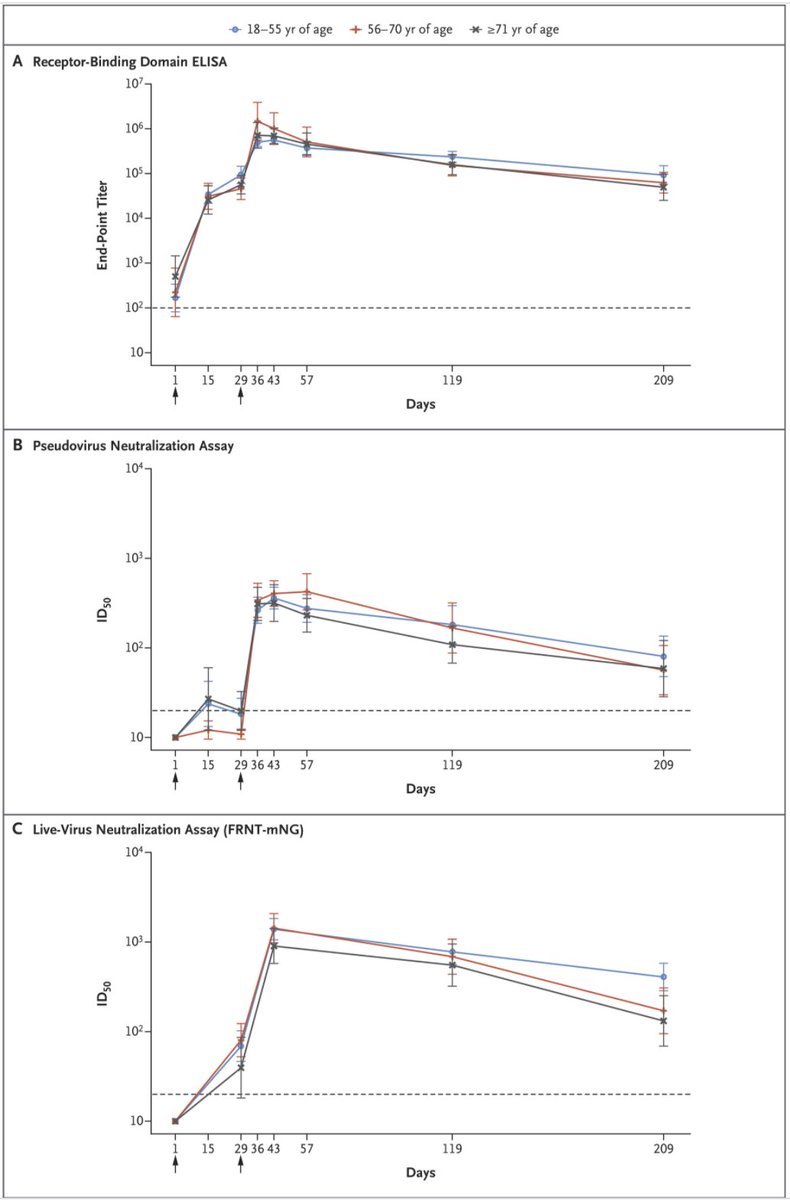
33/ Here’s another study showing that 2nd doses of Moderna vaccine boost antibody levels significantly (day 29 = day of 2nd dose):
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…
34/

35/ Here’s the publication they’re referring to: nature.com/articles/s4157…
This op-ed really got me rethinking my opinon:
This op-ed really got me rethinking my opinon:
https://twitter.com/celinegounder/status/1378081650580586504
36/ But it’s important to note that the this is an op-ed published in a scientific journal, not published research. nature.com/articles/s4157…
This isn't based on modeling or empirical evidence. And they make numerous assumptions.
This isn't based on modeling or empirical evidence. And they make numerous assumptions.
37/ As I’ve argued above, there are very REAL (not theoretical) risks of selecting for new variants with a 2nd dose delay strategy.

38/ We may be observing the benefits of delaying 2nd doses and spreading out first doses now, in the short term. We won't observe the harms of delaying 2nd doses until later, in the longer term.
39/ Here’s an analogy from the world of TB & HIV. For many years, experts debated when to start treatment for HIV in patients who had both TB and HIV.
40/ It was thought that you should treat a patient for TB x months before starting treatment for HIV because patients with TB could develop immune reconstitution inflammatory syndrome (IRIS) if they got antiretroviral therapy and their immune systems got stronger.
41/ This was a real short-term harm of early treatment for HIV in patients with TB and HIV.
42/ But when clinical trials looked at this formally (e.g. the STRIDE Study clinicaltrials.gov/ct2/show/NCT00…), we realized that there was significant mortality benefit to starting treatment for HIV early.
43/ Just as we’re seeing the short-term upside of delaying 2nd doses… the TB docs who treated these patients only saw the short-term downside (IRIS) of early HIV treatment. They didn't see the long-term downside of dying from AIDS.
44/ I worry about complicating vaccine rollout. The President’s Emergency Plan for AIDS Relief state.gov/pepfar/ was in part successful in scaling up treatment for HIV in sub-Saharan Africa was that it was based on simple protocolized treatment algorithms.
45/ The more complicated you make a big public health program, the harder it is to execute. COVID vaccination is the biggest public health program the U.S. has ever taken on.
46/ I disagree with this. The assumption is that people would not die or be harmed by dose delay. We don't know that.
47/ This was also the argument made about letting patients try experimental drugs during the early years of the AIDS pandemic or for loosening the FDA approval process for HIV treatments.
48/ Even some of the most strident HIV activists like @PeterStaley and @TAGTeam_Tweets Mark Harrington understood the importance and necessity of clinical trials to answer these kinds of difficult questions. justhumanproductions.org/podcasts/e10-d…
49/ And so the answer to the question: to delay 2nd doses of the Pfizer and Moderna COVID vaccines? Or not to delay?
50/ It’s a decidedly un-Shakespearean one.
Fear of death makes us all cowards, but we do NOT become weak from study and thought.
We must not delay 2nd doses without first doing the research to support it.
Fear of death makes us all cowards, but we do NOT become weak from study and thought.
We must not delay 2nd doses without first doing the research to support it.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



