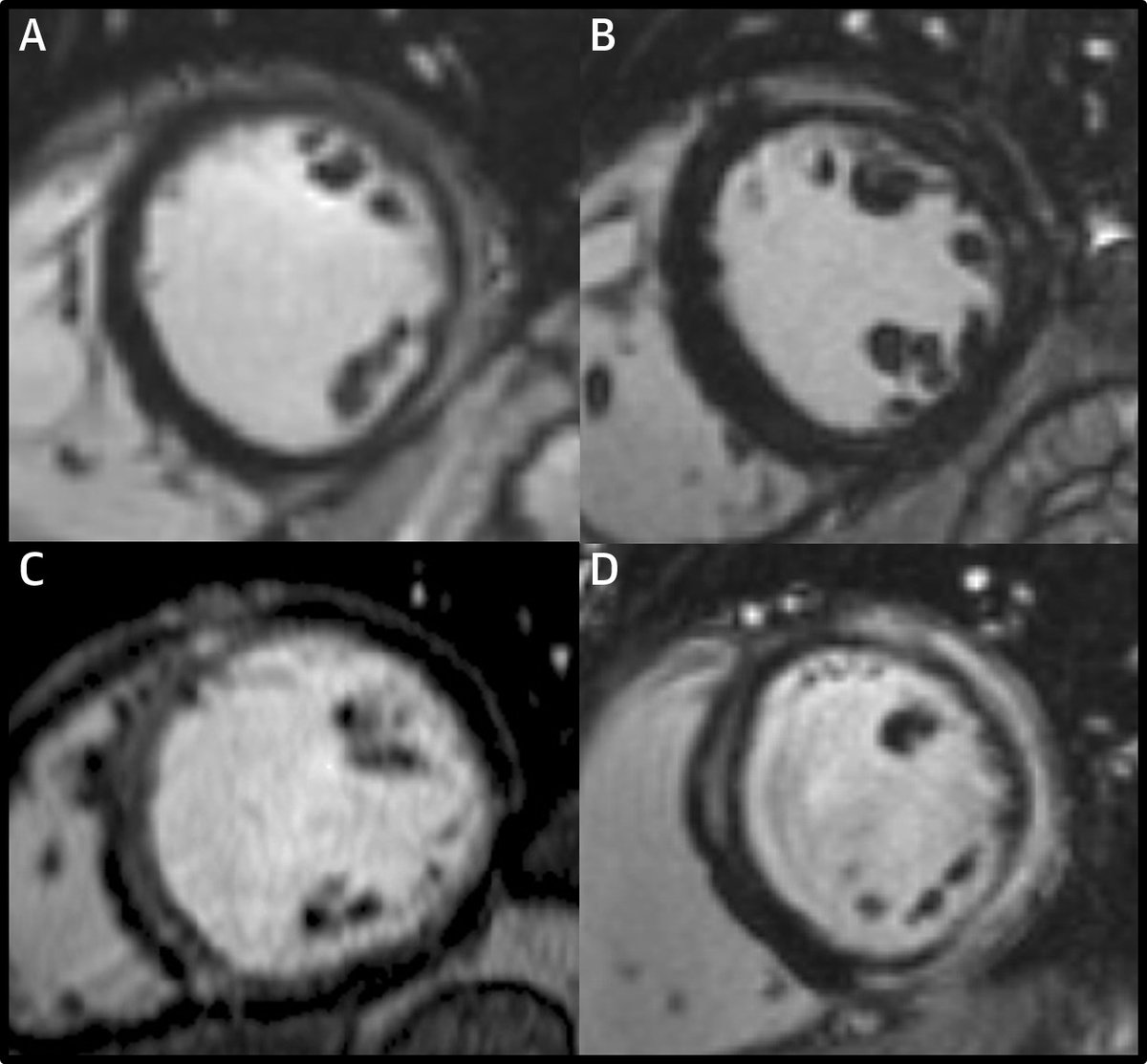
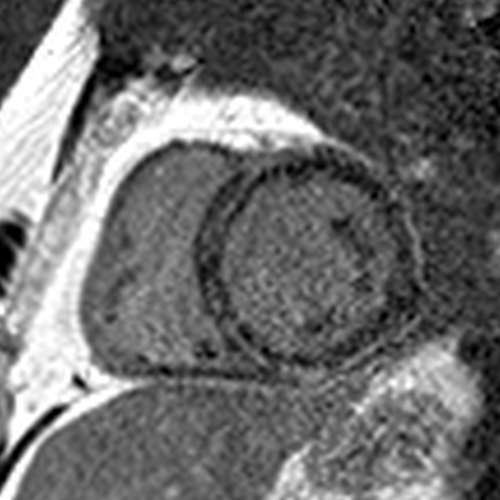
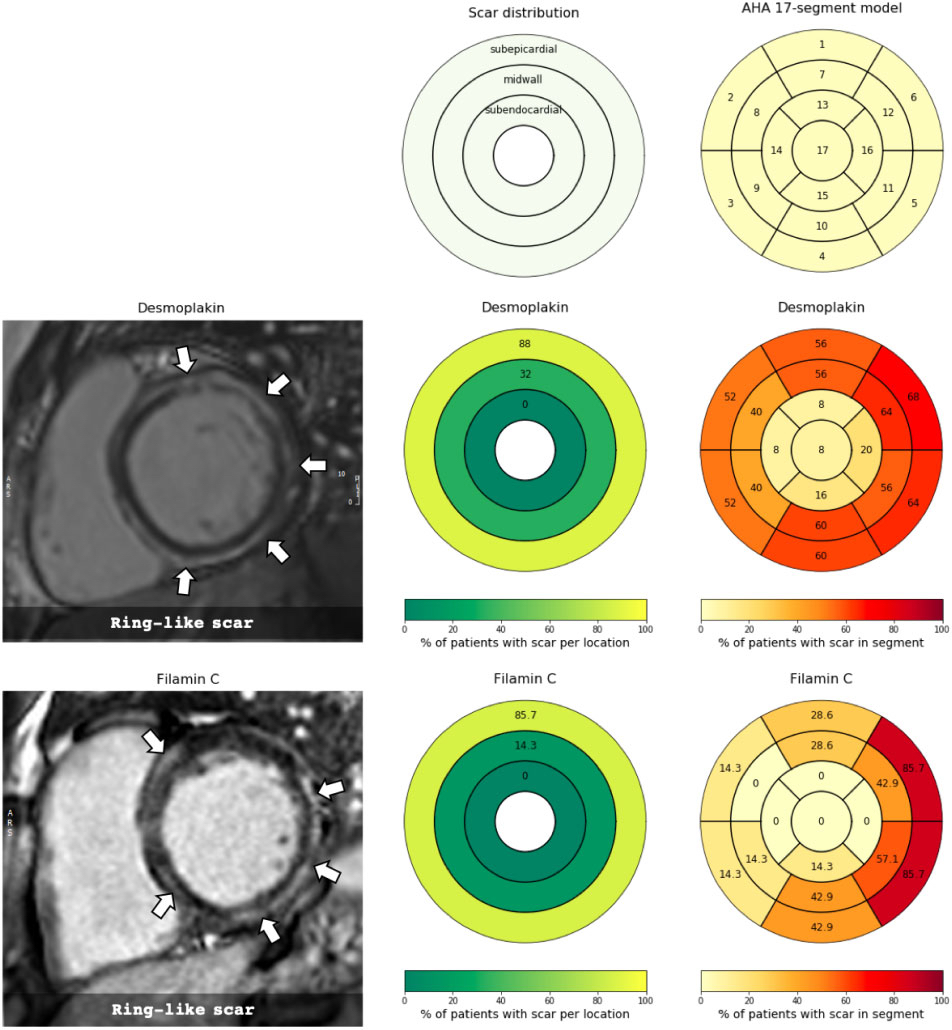
I think it’s genetic ACM because of the pattern of LGE involvement. There is circumferential LGE (the "ring sign") with lateral wall predominance vs. septal (unlike in cardiac sarcoidosis).
https://twitter.com/pnagpalMD/status/1387381414698627072
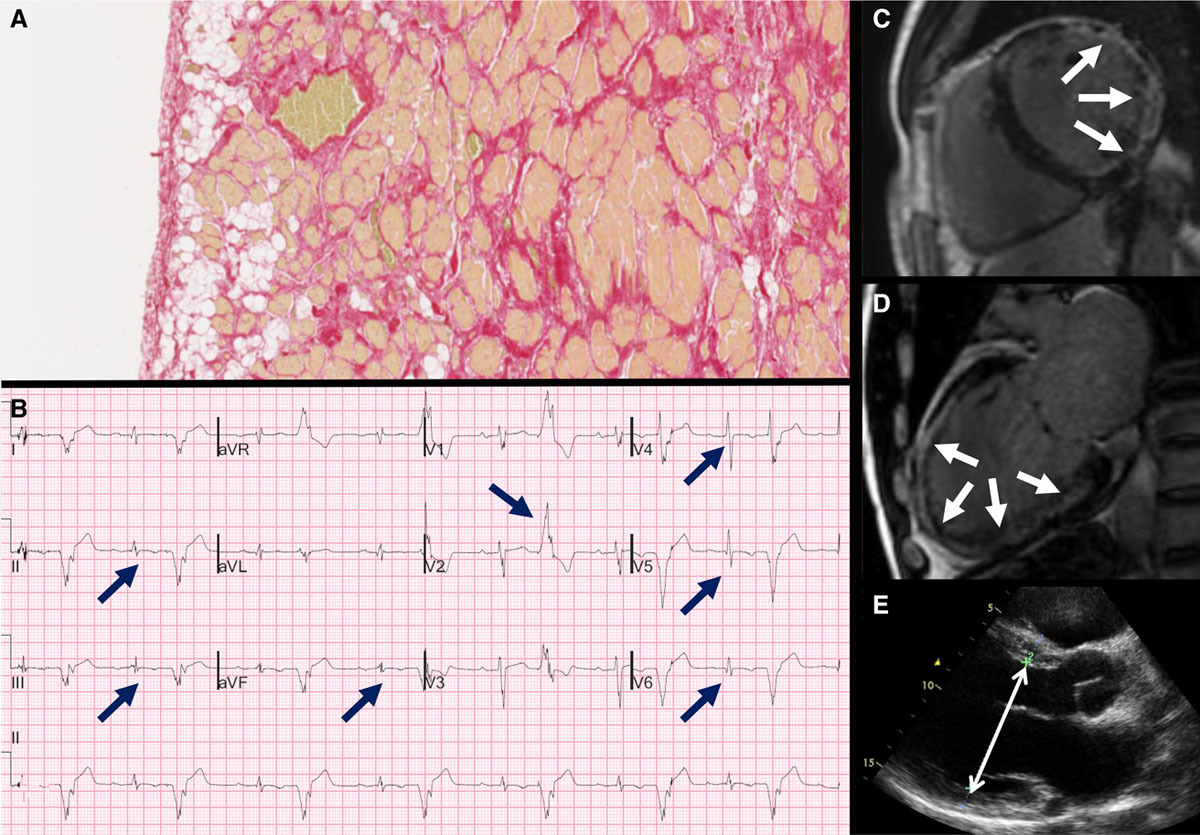
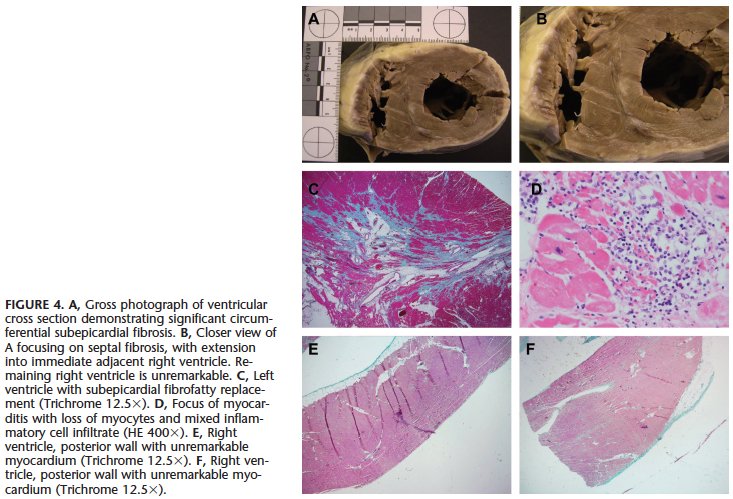
The lateral wall involvement spares the most subendocardial portion and/or the papillary muscles and trabeculations, indicating it is subepicardial (unlike a transmural MI that started subendocardially and involves the papillary muscles/trabeculations). 
In the septum, the LGE spares the very RV side of the septum (also a distinguishing feature from cardiac sarcoidosis) and is therefore often midmyocardial… the ring is subepicardial laterally and midmyocardial septally.
This pattern has been shown in ACM in pathology studies such as these:
ahajournals.org/doi/10.1161/CI…
pubmed.ncbi.nlm.nih.gov/19465822/
ahajournals.org/doi/10.1161/CI…
pubmed.ncbi.nlm.nih.gov/19465822/
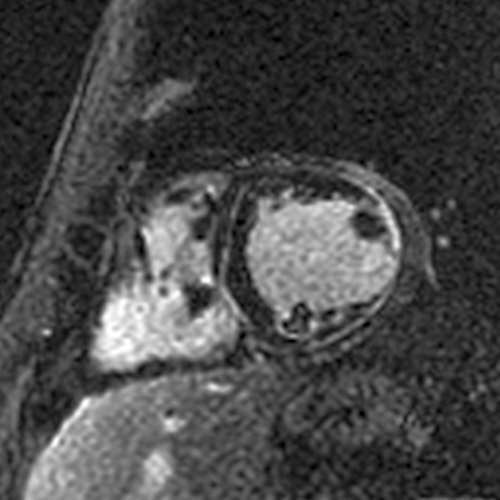
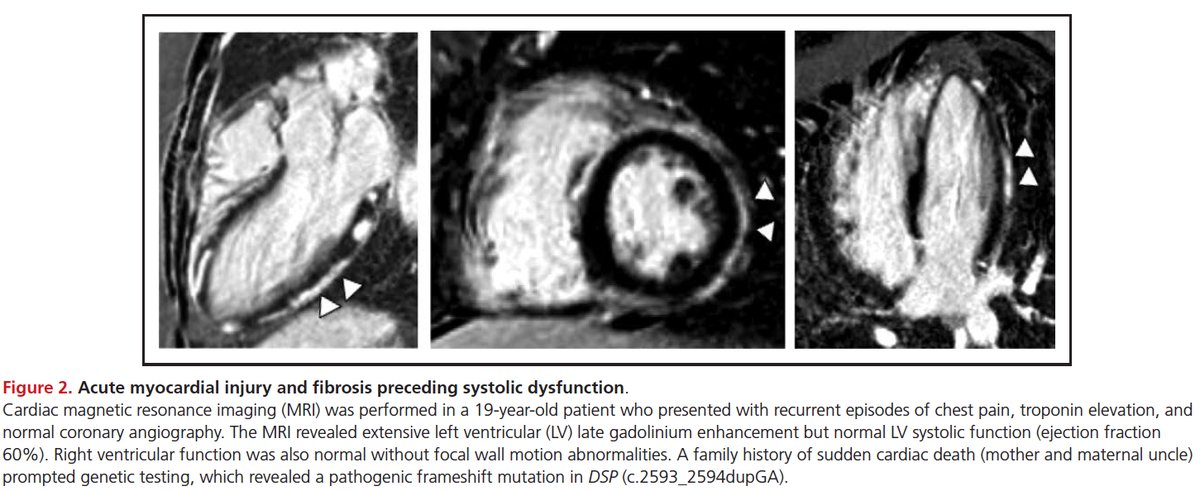
Elevated T1/T2 indicates an acute process (myocarditis), but it does not indicate the *cause*. We know ACM can present with acute myocarditis... this is one recent study:
ahajournals.org/doi/full/10.11…
ahajournals.org/doi/full/10.11…
The fact that genetic ACM can present with myocarditis is not new... it has been described for 15-20 years. For example, here’s a sentence from a 2008 paper from the legendary Bill McKenna:
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…

Resolution of LGE does not tell us the cause of the myocarditis… it is simply a function of the extent of acute injury. Acute injury of a smaller extent can heal and become undetectable by LGE (= the scar is under the threshold of detection).
Bottomline – a diagnosis of myocarditis (like a diagnosis of NICM) is not wrong, but it’s incomplete. Not all myocarditis is viral.
We have a growing database of ACM cases, some with myocarditis... we hope to publish our experience at some point.
We have a growing database of ACM cases, some with myocarditis... we hope to publish our experience at some point.
• • •
Missing some Tweet in this thread? You can try to
force a refresh