First, was the LGE in this study an artifact ("overcalling")?
No, because:
- This paper comes from pioneers and some of the biggest names in CMR
- Our anecdotal experience matches these findings
- The images in the paper very clearly demonstrate LGE.
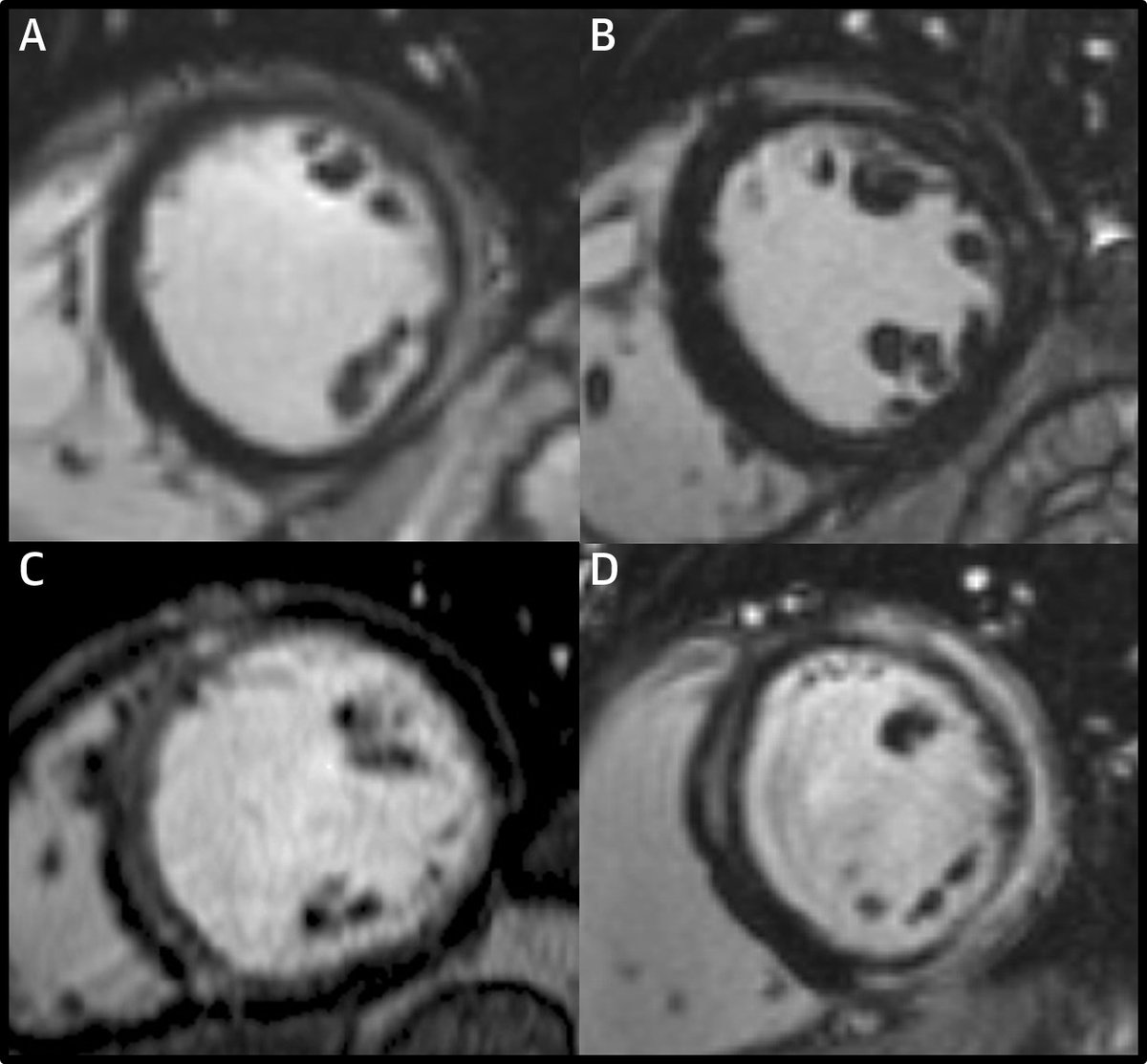
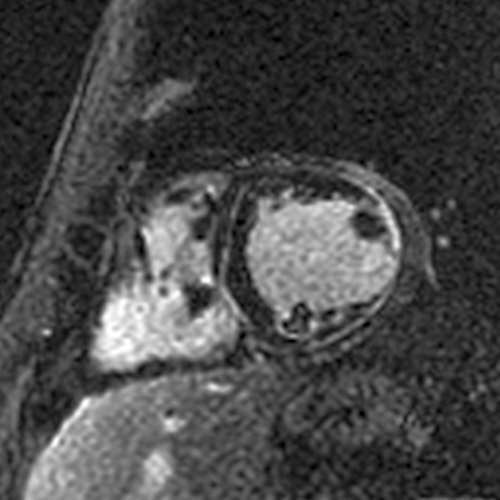
I think it’s genetic ACM because of the pattern of LGE involvement. There is circumferential LGE (the "ring sign") with lateral wall predominance vs. septal (unlike in cardiac sarcoidosis).
The lateral wall involvement spares the most subendocardial portion and/or the papillary muscles and trabeculations, indicating it is subepicardial (unlike a transmural MI that started subendocardially and involves the papillary muscles/trabeculations).
May 19, 2020 • 28 tweets • 7 min read
It’s been over 2 months since the first descriptions of cardiac manifestations of Covid-19. There have been many papers and reviews on this topic. What have we learned about how SARS-CoV-2 can affect the heart? #whyCMR#cardiotwitter
Troponin elevations and low EFs are frequently described. Why do they happen? Most papers use the term Covid-19 myocarditis. But can SARS-CoV-2 cause fulminant myocarditis (= extensive focal myocardial necrosis, as seen with viral lymphocytic or giant cell myocarditis)?
Nov 12, 2019 • 13 tweets • 3 min read
Here’s an interesting paper published in JACC yesterday. The investigators studied 187 acute myocarditis patients with CMR (within a week) and repeated the CMR at 6 months. onlinejacc.org/content/74/20/…
They found that LGE was present in 96% at the initial presentation and 86% at 6 months. They conclude:
“In the acute setting, LGE does not mean definite fibrosis, and it may disappear at 6 months.”
Aug 24, 2019 • 18 tweets • 4 min read
With all the discussion about viability in the past few days, I would like to share how I interpret and report viability on CMR. I first look for LGE. Rarely, there’s no LGE and it’s all viable or more likely, a non-ischemic cardiomyopathy. #WhyCMR 1/18
When I see LGE, I confirm it’s in an ischemic pattern – subendocardial or transmural, and limited to a coronary territory, i.e., an MI. If not, it's again a non-ischemic cardiomyopathy and not a viability issue anymore. 2/18