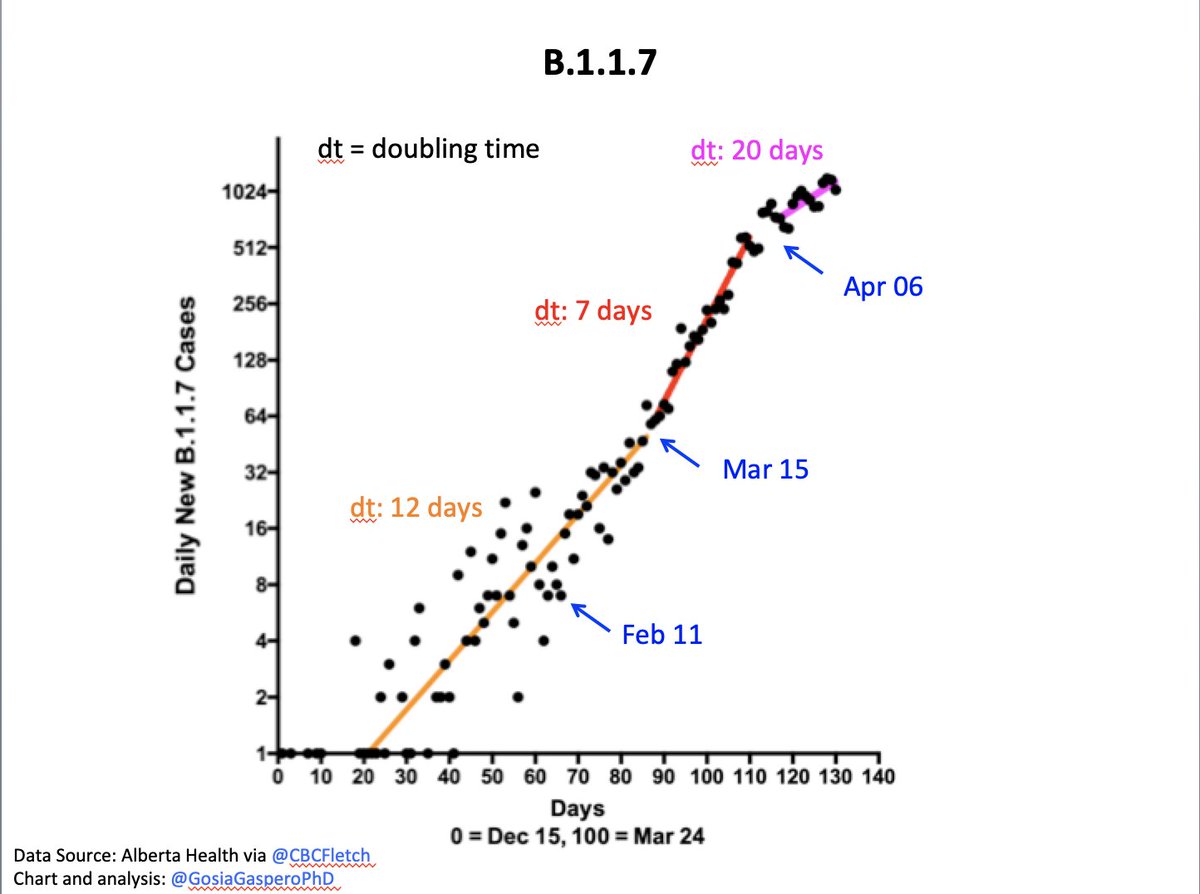
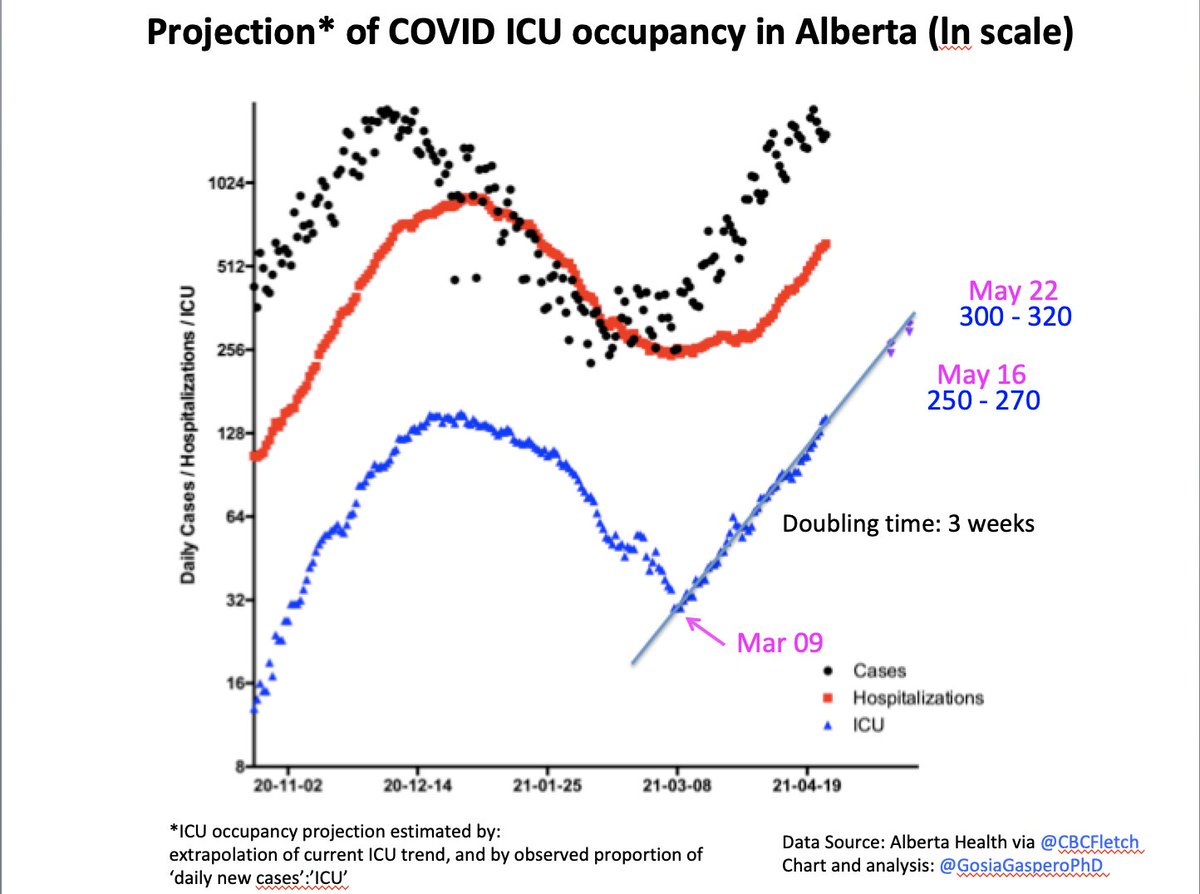
Alberta: Current measures made the growth rate less extreme.
B117 is doubling now every 20 days instead of every 7 days.
It's still very fast - similar to doubling time in the 2nd wave (18 days)
Current measures are insufficient to bend the curve downwards.
Ln scale graph 👇
B117 is doubling now every 20 days instead of every 7 days.
It's still very fast - similar to doubling time in the 2nd wave (18 days)
Current measures are insufficient to bend the curve downwards.
Ln scale graph 👇
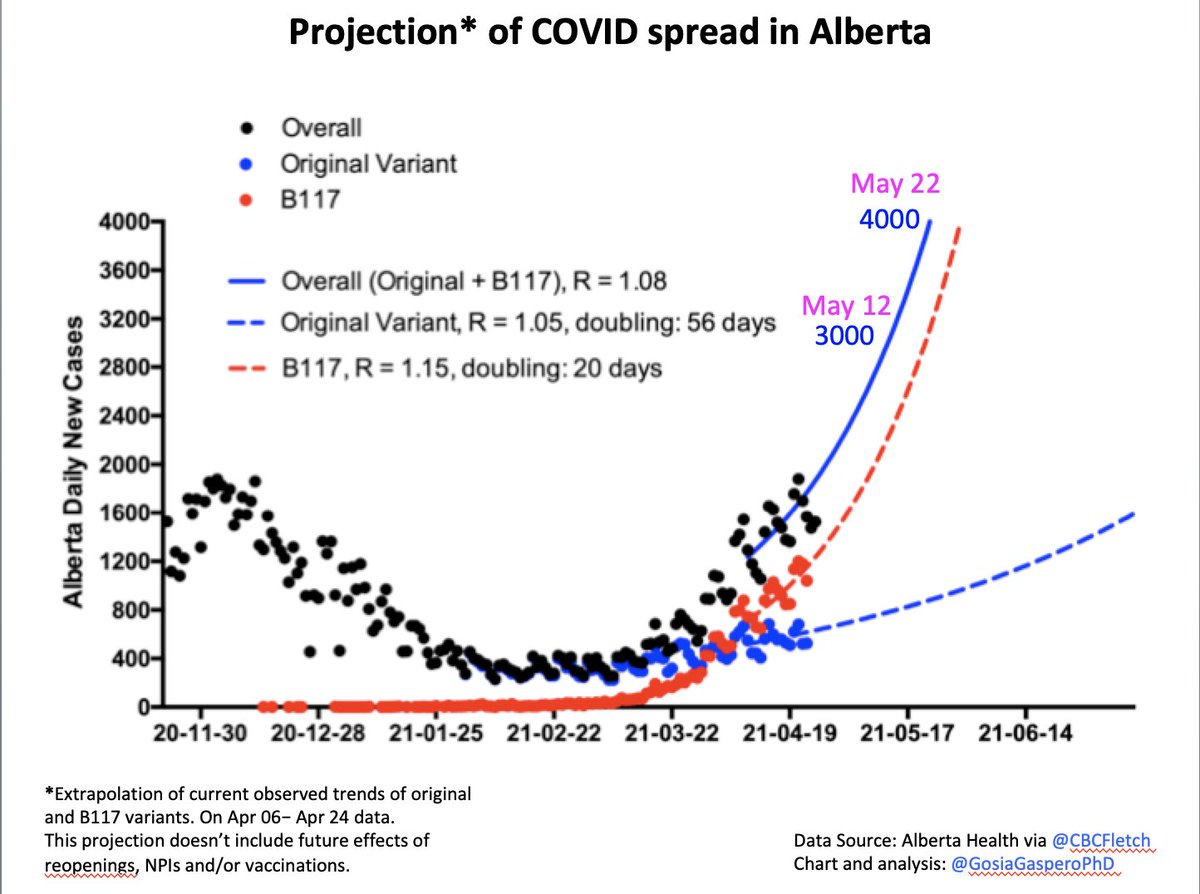
At this rate we can expect:
3,000 daily new cases on May 12
4,000 daily new cases on May 22
2/
3,000 daily new cases on May 12
4,000 daily new cases on May 22
2/
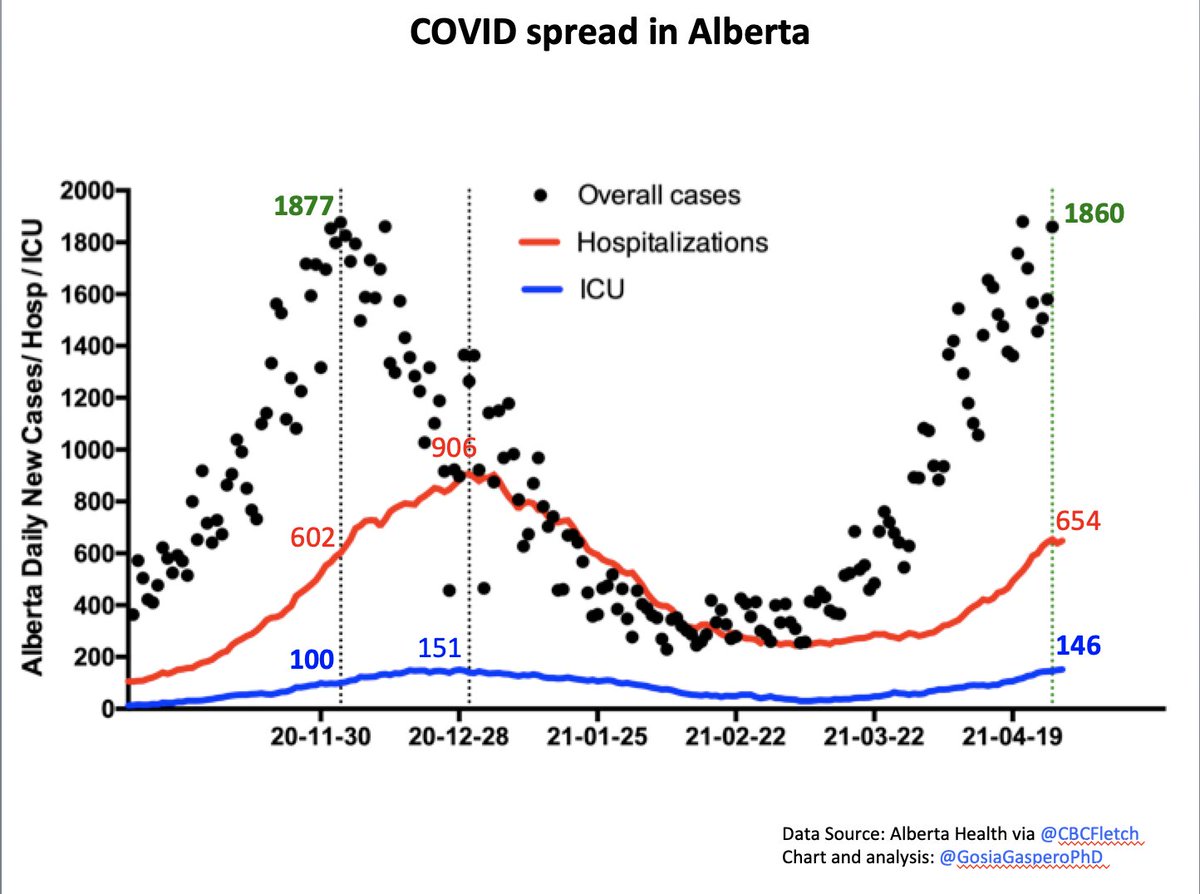
This wave is worse than the fall one.
2nd wave: at 1877 daily cases we had 100 ICUs
3rd wave: at 1860 daily cases we have 146 ICUs, and *we are still growing*
That's *despite* many people being already vaccinated. W/o vaccines it would be even worse.
3/
2nd wave: at 1877 daily cases we had 100 ICUs
3rd wave: at 1860 daily cases we have 146 ICUs, and *we are still growing*
That's *despite* many people being already vaccinated. W/o vaccines it would be even worse.
3/
COVID-ICU numbers grow in a clear exponential fashion since Mar 09. Doubling every 3 weeks.
At this rate we may expect:
May 16, 250-270 ICUs
May 22, 300-320 ICUs
4/
At this rate we may expect:
May 16, 250-270 ICUs
May 22, 300-320 ICUs
4/
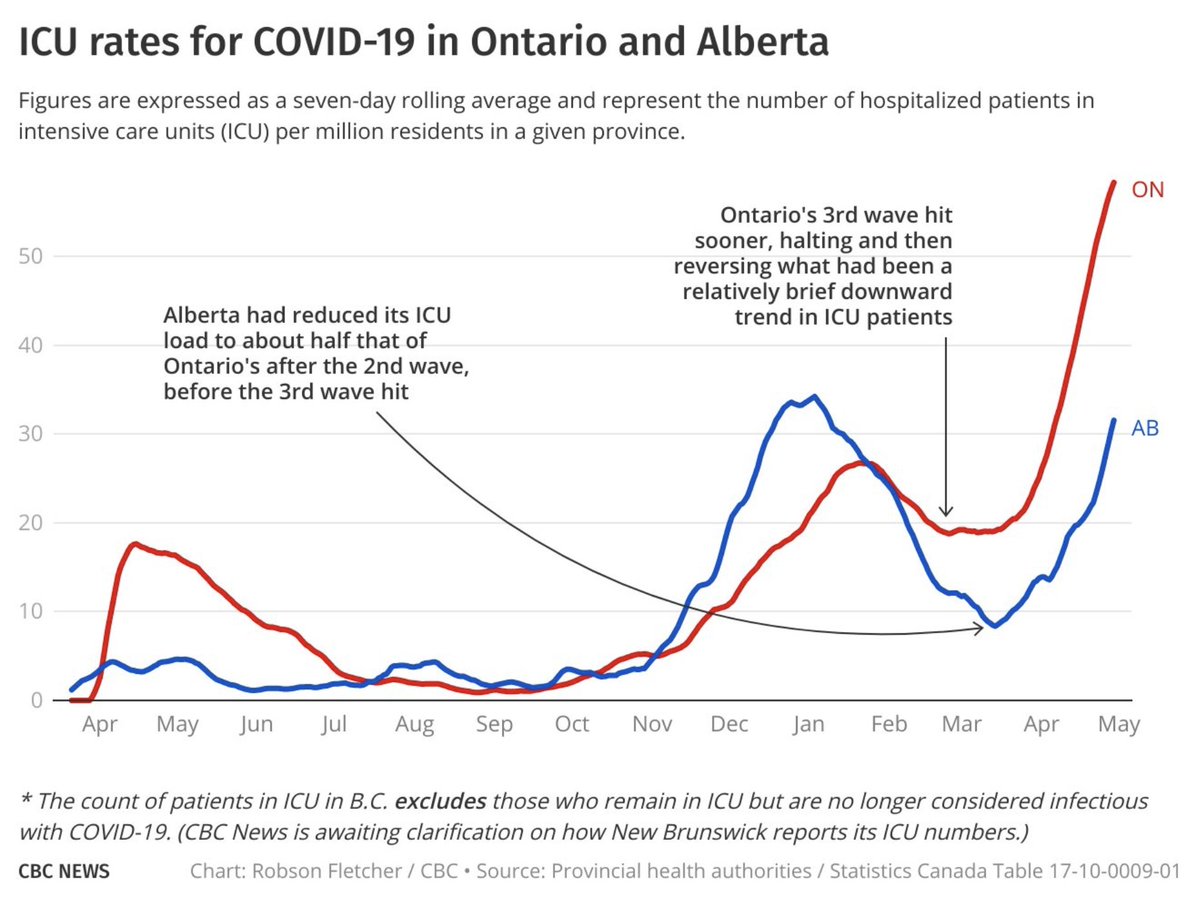
"Oh, but we are not like Ontario."
Well, not yet. We started at lower ICU numbers. But we are on exactly the same steep upward trajectory as ON.
Excellently explained by @CBCFletch 👇
5/
Well, not yet. We started at lower ICU numbers. But we are on exactly the same steep upward trajectory as ON.
Excellently explained by @CBCFletch 👇
5/
https://twitter.com/CBCFletch/status/1387952217576116228?s=20
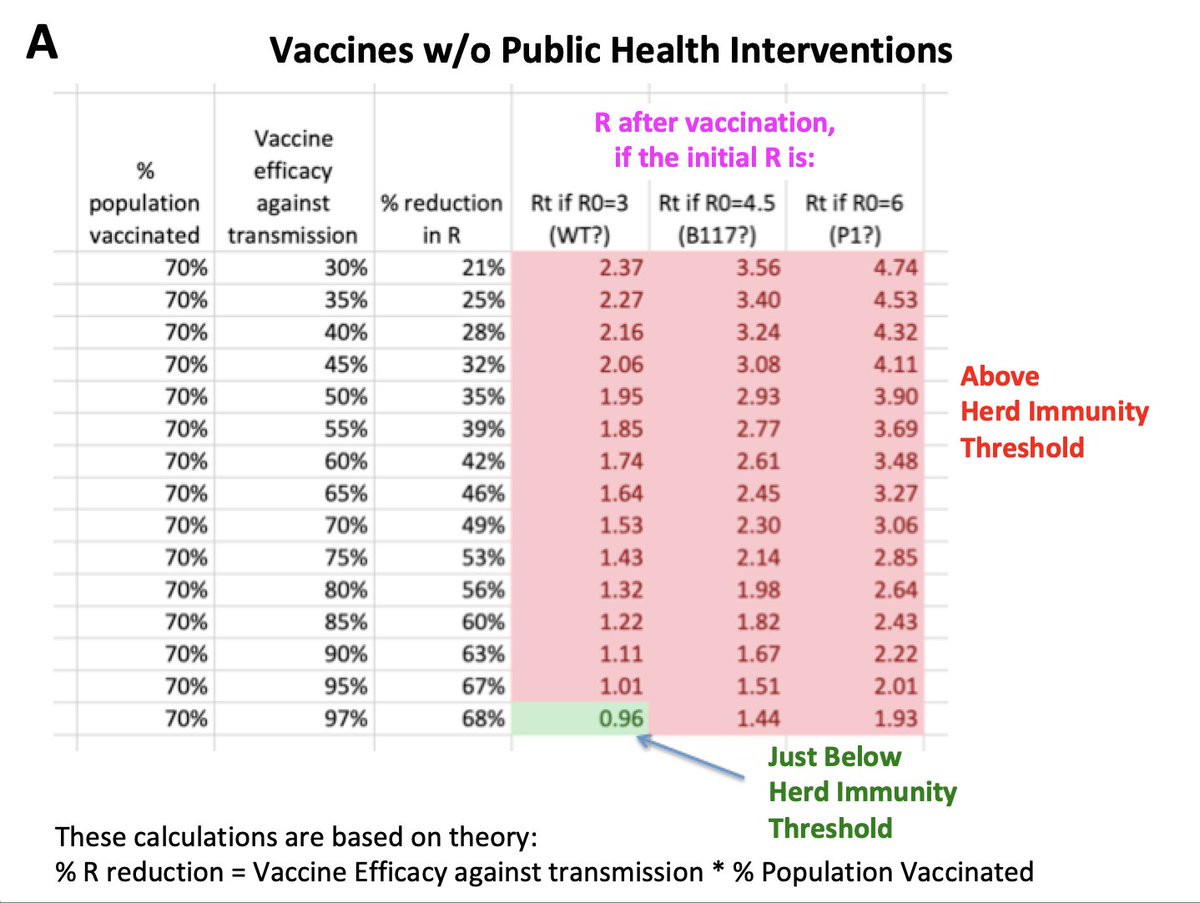
Re Vaccines and the "Best Summer Ever":
W/o public health measures vaccines most likely won't end the pandemic (A)
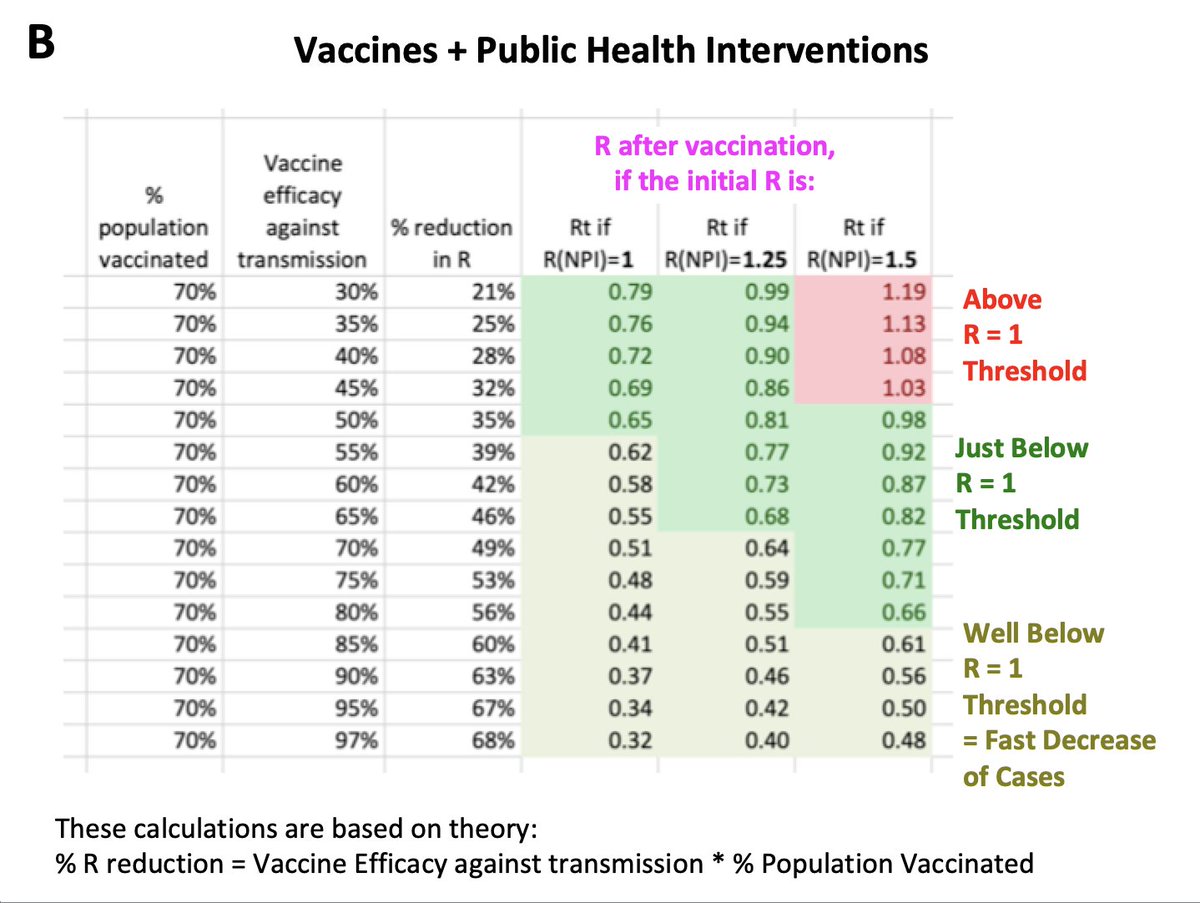
W/ public health measures vaccines are an amazing tool to help us *stop the virus spread* very fast (B)
@ R=0.5 one can get from 1000 daily cases to 0 in just 40d
W/o public health measures vaccines most likely won't end the pandemic (A)
W/ public health measures vaccines are an amazing tool to help us *stop the virus spread* very fast (B)
@ R=0.5 one can get from 1000 daily cases to 0 in just 40d
The only way to get us out of the pandemic and get the relative normalcy back is to aim for Covid elimination.
Please sign the ZeroCOVIDCanada Open Letter addressed to federal and provincial governments 👇zerocovidcanada.org/take-action
Please sign the ZeroCOVIDCanada Open Letter addressed to federal and provincial governments 👇zerocovidcanada.org/take-action
• • •
Missing some Tweet in this thread? You can try to
force a refresh