
THREAD on B1617 from COG data:
Yesterday I did some tweets about the growth of B1617 ("India") and its subtypes in the community using data from the Sanger Inst (England only).
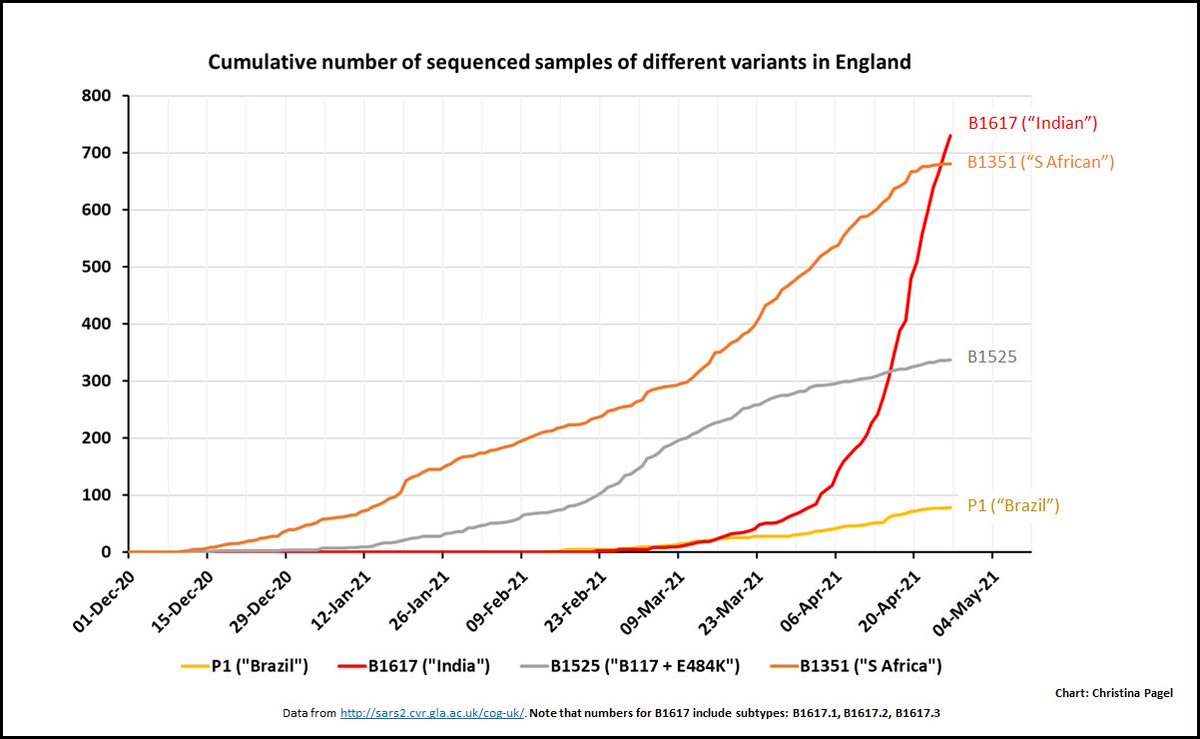
Here is the recent data from England from COG (genetics consortium for covid)
Yesterday I did some tweets about the growth of B1617 ("India") and its subtypes in the community using data from the Sanger Inst (England only).
https://twitter.com/chrischirp/status/1389349904770813957?s=20
Here is the recent data from England from COG (genetics consortium for covid)
2.This includes data from travellers & surge testing
BUT overall picture is the same as for community cases from Sanger yesterday.
B1617 growing very fast & has overtaken all other variants of concern / under investigation (except B117 ("Kent") which is still >90% of cases).
BUT overall picture is the same as for community cases from Sanger yesterday.
B1617 growing very fast & has overtaken all other variants of concern / under investigation (except B117 ("Kent") which is still >90% of cases).
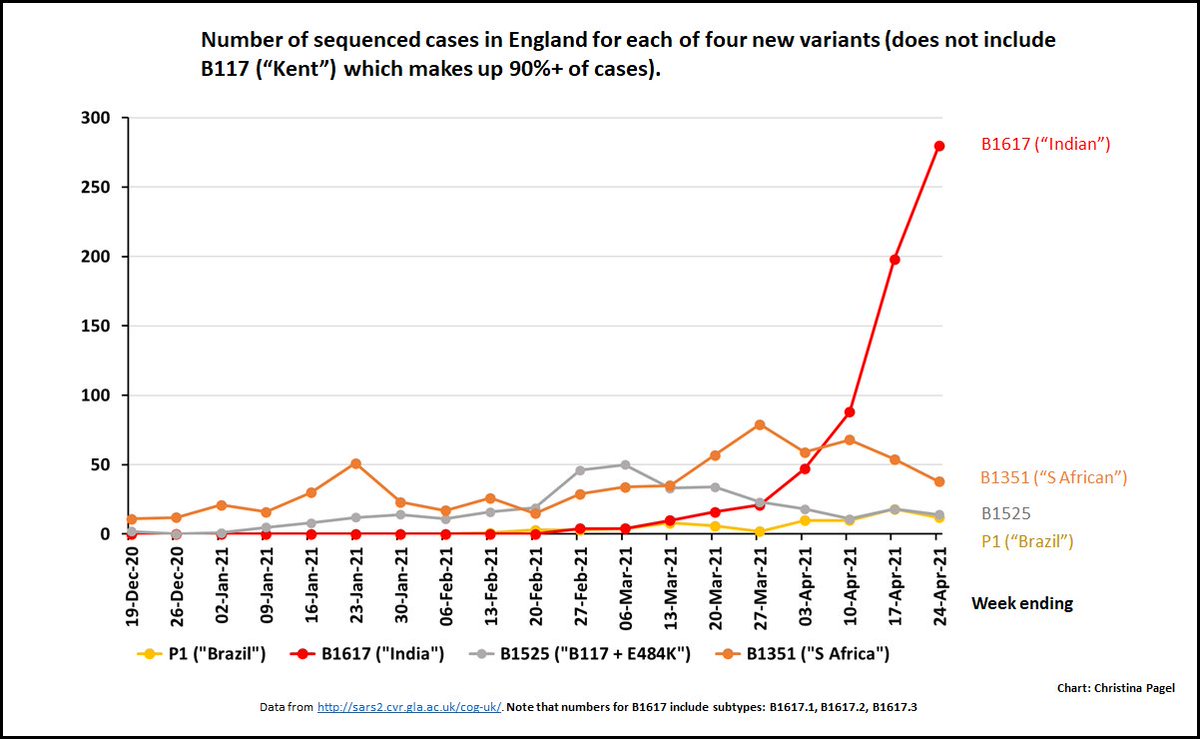
3.Look at the number each week, you can see that the other main variants are hardly growing. B117 cases ("Kent") are also going down (which is why our overall case numbers are falling).
But this variant, B1617 ("India"), is still shooting up.
But this variant, B1617 ("India"), is still shooting up.
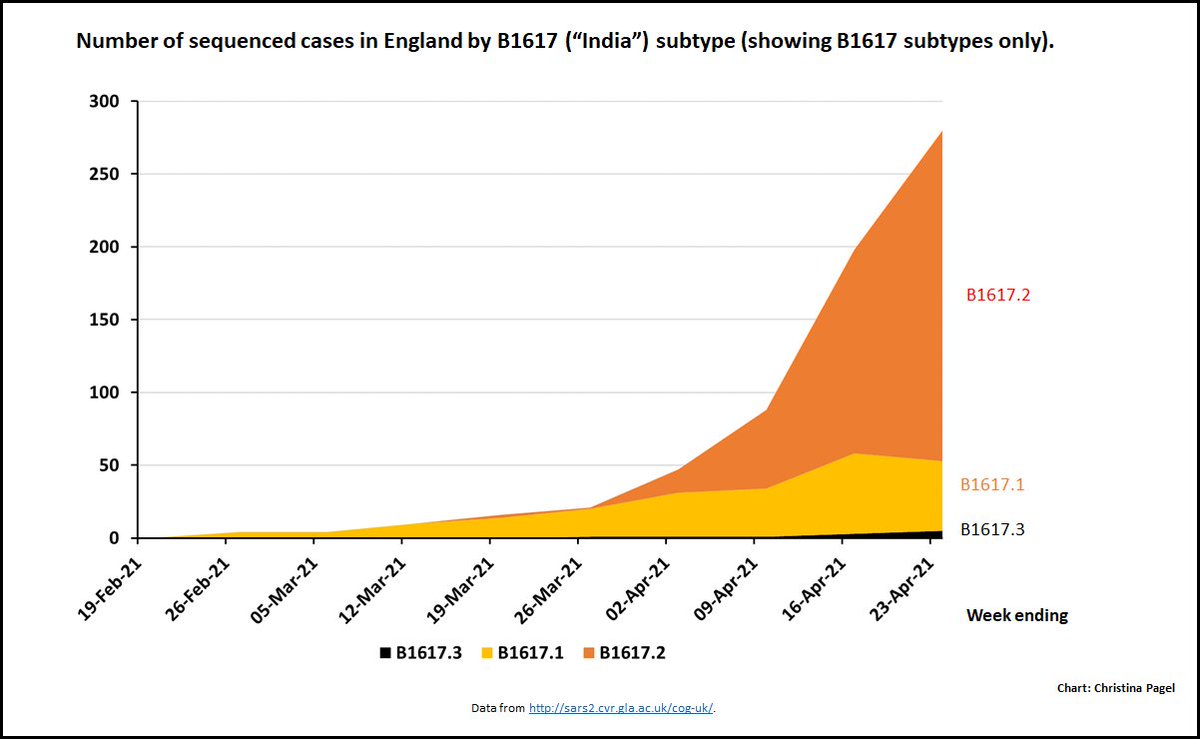
4.Digging into its subtypes, one in particular stands out: B.1617.2.
This is the one *without* the E484Q mutation. It is *also* the sub-strain that is now dominating India.
This is the one *without* the E484Q mutation. It is *also* the sub-strain that is now dominating India.
5.Who knows why it's outcompeting its variant siblings... (I don't anyway). Perhaps the prelim data from @GuptaR_lab showing that the "E484Q"+"L452R" mutations didn't seem to confer any advantage over just "L452R" provides a clue?
https://twitter.com/GuptaR_lab/status/1388422662595219459?s=20
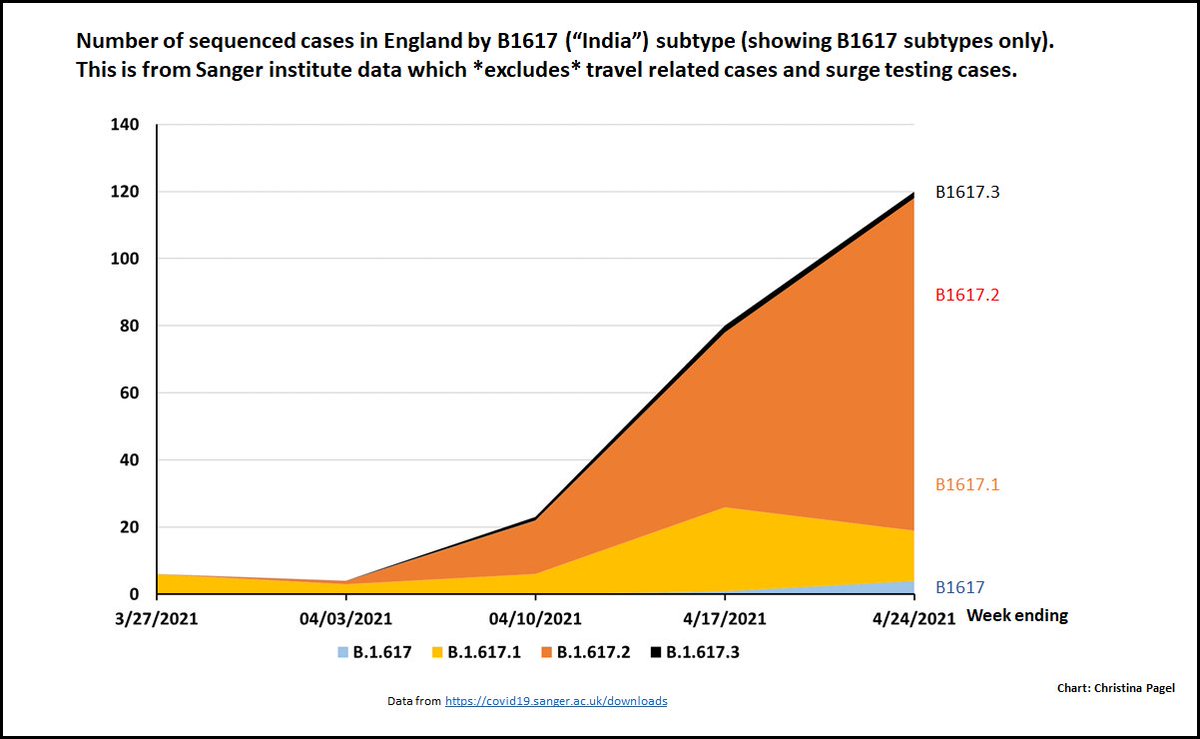
6.But basically - we've seen this characteristic spread in India, we are seeing it in the COG data (all England data - tweet 4 above) and we are seeing it in the Sanger data (just community cases).
Sanger chart is below
Sanger chart is below
7. Do we have definitive evidence that B1617.2 is more transmissible? No
But honestly I think canaries are chirping - we know it's in the community (from Sanger) and we should act to contain right now while numbers manageable. /END
But honestly I think canaries are chirping - we know it's in the community (from Sanger) and we should act to contain right now while numbers manageable. /END
• • •
Missing some Tweet in this thread? You can try to
force a refresh






















