FND in the Emergency Department. A new review for @AcademicEmerMed with Sara Finkelstein, Miguel (ED) and Achelle (Neuro) Cortel-LeBlanc. Open access - onlinelibrary.wiley.com/doi/full/10.11…. A quick thread , especially for ED folks 1/.. 
FND is one of the commonest neurological problems in the ED. At least 10% of all seizures in the ED and around 50% of ‘status’ presentations. 9% of all stroke presentations in London. 9% of all acute neurology admissions in NZ. 2/
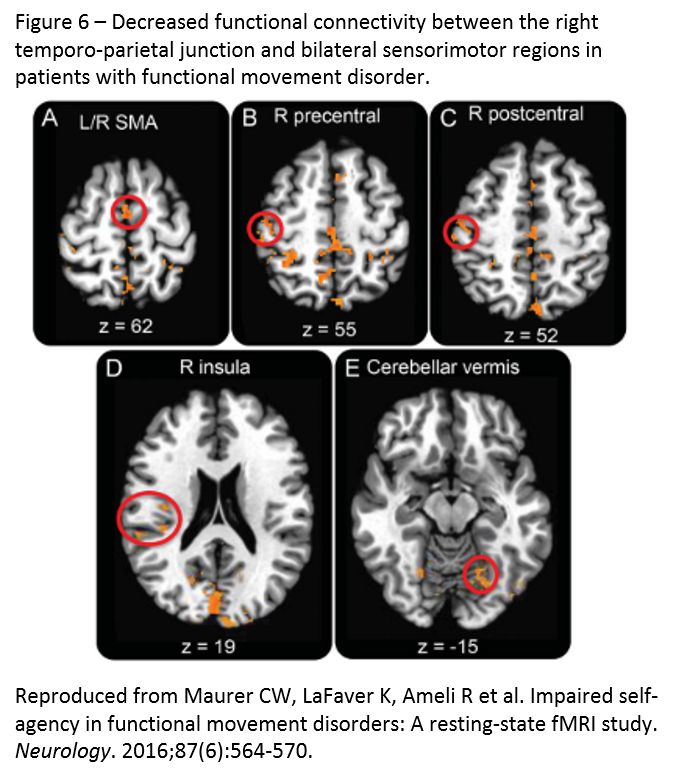
FND is a problem at the interface between neurology and psychiatry. It has its own unique neurobiology. This international review just out in the last couple of weeks. 3/ sciencedirect.com/science/articl…
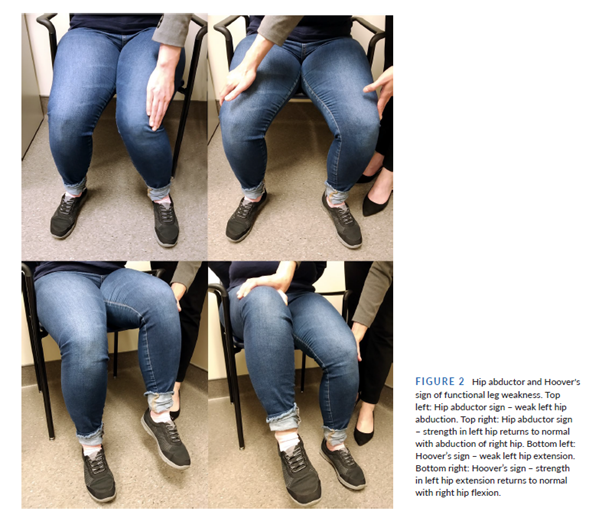
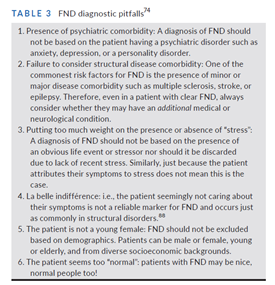
FND is a 'rule in' diagnosis. If you are making the diagnosis just because tests are normal, or because you don’t know what else to call it – you’re doing it wrong. 4/
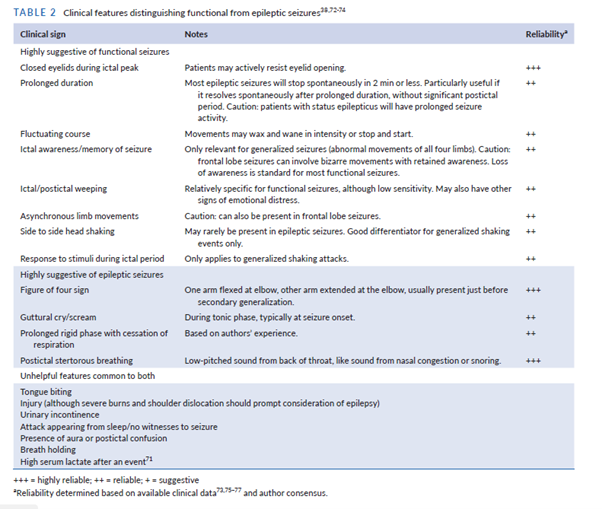
Functional Seizures also have a range of typical features. Every year around the world there must be thousands of patients with FND who are needlessly intubated because FND is not properly on clinicians radar. Here are some clues 5/
Recent work also shows that most people with suspected cauda equina syndrome will have normal or non-explanatory imaging. Do the MRI urgently, but if inormal, think about FND – as this appears to be common in this patient group. n.neurology.org/content/96/3/e…
FND usually needs a neurologist, or someone used to neurological diagnosis, to confirm the diagnosis. There are many pitfalls. But that doesn’t mean you cant list FND on your differential like any other medical condition 7/
FND is genuine, not ‘faking’. We know that does happen, especially in ED, but be REALLY careful. Its rare for those of us who see these patients in neurology settings to encounter feigned symptoms. 8/
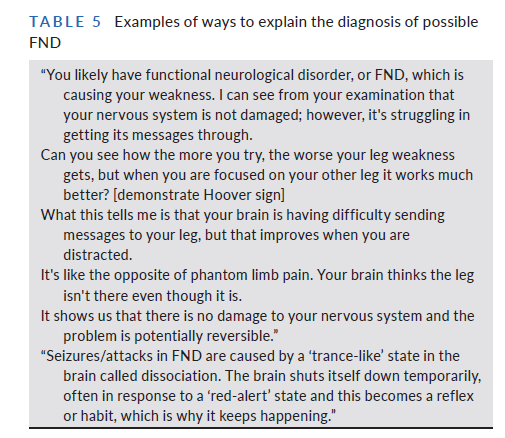
If you are dealing with FND in an ED setting, especially perhaps if the diagnosis has been made elsewhere, there are ways of communicating the diagnosis that are truthful and can help lay the groundwork for rehabilitation treatment. 9/
To learn more about FND have a look at neurosymptoms.org, fndhope.org, fndaction.org.uk and @fndportal's pinned 'thread of threads'. Heres another thread dealing with ten myths of FND.
https://twitter.com/jonstoneneuro/status/1268626216040501252?s=20. END
And not forgetting @fndsociety now with over 800 members and weekly free webinars. Join for the back catalogue of over 30 talks and a meeting planned for Boston 2022
• • •
Missing some Tweet in this thread? You can try to
force a refresh