
1/9
👉 Some tips for a safer, faster, and easier EUS-gastroenterostomy (EUS-GE)
✴️an interventional EUS procedure used for malignant gastric outlet obstruction✴️
#EUS #AdvancedEndo #GITwitter
(All media posted with permission)
👉 Some tips for a safer, faster, and easier EUS-gastroenterostomy (EUS-GE)
✴️an interventional EUS procedure used for malignant gastric outlet obstruction✴️
#EUS #AdvancedEndo #GITwitter
(All media posted with permission)
2/9
👉Patient selection is key
✔️If life expectancy is < 3 months, we believe risks of EUS-GE outweigh benefits ➡️choose duodenal stent
✔️ If > 3 months, go for EUS-GJ
@BilalMohammadMD @NickMcDonaldMD
ncbi.nlm.nih.gov/pmc/articles/P…
👉Patient selection is key
✔️If life expectancy is < 3 months, we believe risks of EUS-GE outweigh benefits ➡️choose duodenal stent
✔️ If > 3 months, go for EUS-GJ
@BilalMohammadMD @NickMcDonaldMD
ncbi.nlm.nih.gov/pmc/articles/P…
3/9
👉Study pre-procedural imaging carefully
✔️ You want to see a distended stomach with D3/D4 coursing immediately inferior to and adjacent to gastric body
In this CT slice, the IR placed GJ tube is a nice guide as to how D3/D4 courses in relation to the stomach
👉Study pre-procedural imaging carefully
✔️ You want to see a distended stomach with D3/D4 coursing immediately inferior to and adjacent to gastric body
In this CT slice, the IR placed GJ tube is a nice guide as to how D3/D4 courses in relation to the stomach

4/9
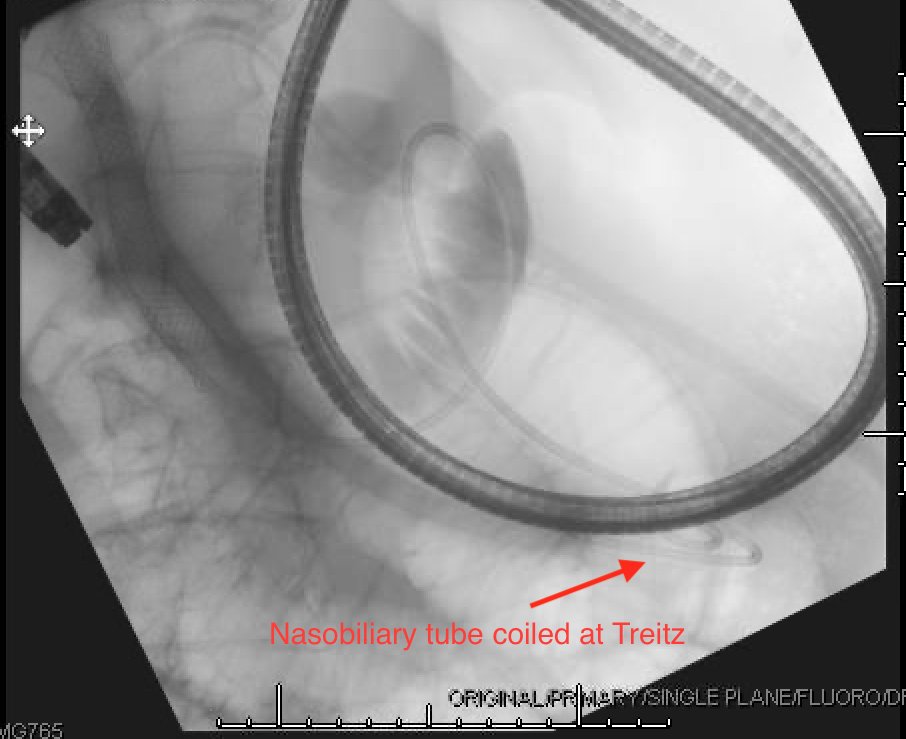
👉Place the pigtail of your naso-biliary drain at the ligament of Treitz
✔️ This is your ideal puncture site to maximize your window for deep insertion of LAMS catheter (which will minimize AEs)
✔️Connect NB drain to water pump and infuse saline, contrast, and methylene blue
👉Place the pigtail of your naso-biliary drain at the ligament of Treitz
✔️ This is your ideal puncture site to maximize your window for deep insertion of LAMS catheter (which will minimize AEs)
✔️Connect NB drain to water pump and infuse saline, contrast, and methylene blue
5/9
👉Use fluoro to guide EUS-scope to ligament of Treitz
✔️ On EUS, this is where you will find your best window with a long "runway" to hub your LAMS catheter and ensure complete opening of the distal flange (4.7cm here!)
✔️ Continue to infuse fluid up until moment you puncture
👉Use fluoro to guide EUS-scope to ligament of Treitz
✔️ On EUS, this is where you will find your best window with a long "runway" to hub your LAMS catheter and ensure complete opening of the distal flange (4.7cm here!)
✔️ Continue to infuse fluid up until moment you puncture

6/9
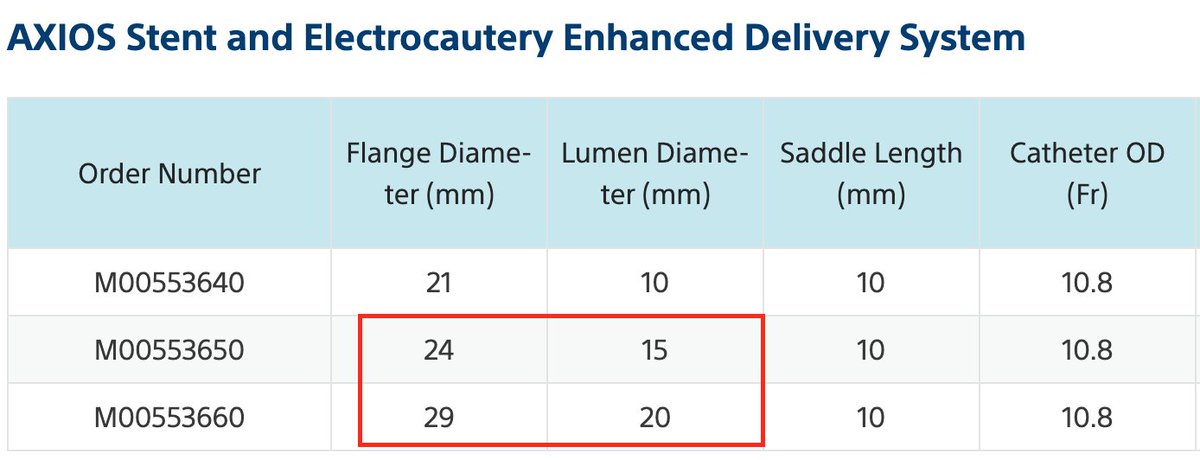
👉 Use a 15mm, not a 20mm LAMS
✔️Anecdotal experience suggests that patients with a 15mm stent do just as well and can tolerate a near regular diet
✔️The outer flange diameter of 24mm vs 29mm gives you a larger margin of error to fully open distal flange in a tight space
👉 Use a 15mm, not a 20mm LAMS
✔️Anecdotal experience suggests that patients with a 15mm stent do just as well and can tolerate a near regular diet
✔️The outer flange diameter of 24mm vs 29mm gives you a larger margin of error to fully open distal flange in a tight space
7/9
👉Always puncture freehand, never over a wire
✔️ Slow and steady (not like an FNA), let the cautery do the work
✔️ Deploy distal flange only when catheter within a thumbs length of being hubbed
✔️Deploy proximal flange in scope➡️big wheel away ➡️unlock catheter➡️push LAMS out
👉Always puncture freehand, never over a wire
✔️ Slow and steady (not like an FNA), let the cautery do the work
✔️ Deploy distal flange only when catheter within a thumbs length of being hubbed
✔️Deploy proximal flange in scope➡️big wheel away ➡️unlock catheter➡️push LAMS out
8/9
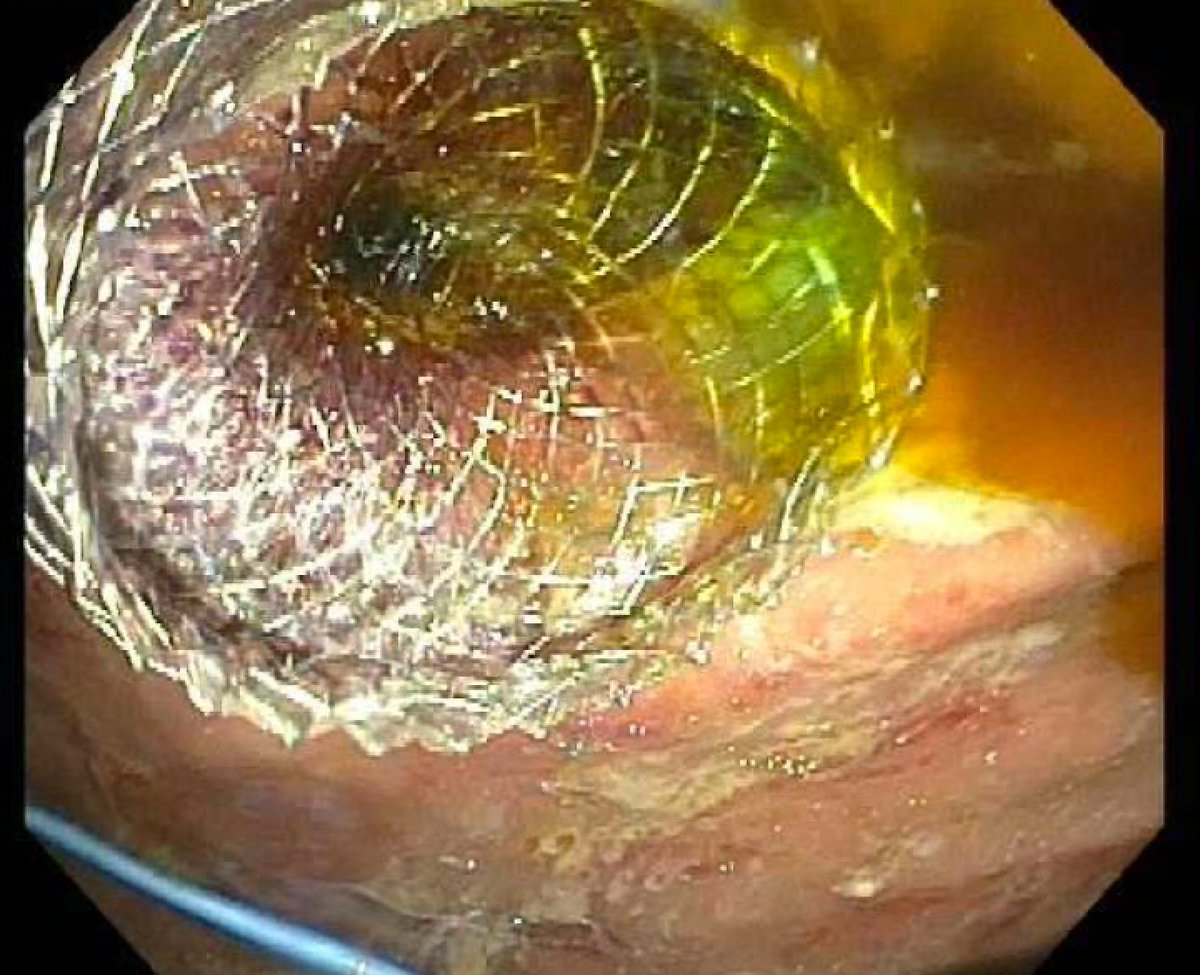
👉Hold your breath, and wait for the methylene blue
Congratulations‼️ 👏
👉Hold your breath, and wait for the methylene blue
Congratulations‼️ 👏
9/9
Of course, EUS-GE should only be performed in expert hands where surgical backup is readily available
Anticipate problems and how to troubleshoot. This is a great video by Shayan Irani highlighting various rescue maneuvers (learn.asge.org ➡️ 2018 DDW Videos)
Of course, EUS-GE should only be performed in expert hands where surgical backup is readily available
Anticipate problems and how to troubleshoot. This is a great video by Shayan Irani highlighting various rescue maneuvers (learn.asge.org ➡️ 2018 DDW Videos)
• • •
Missing some Tweet in this thread? You can try to
force a refresh


