
THREAD - my thoughts on variant situation:
I've been tweeting about it a lot but much has happened in last day.
@guardian today quoted me saying that my personal feeling was we should delay next stage of Roadmap.
theguardian.com/world/2021/may…
Let me explain why... 1/18
I've been tweeting about it a lot but much has happened in last day.
@guardian today quoted me saying that my personal feeling was we should delay next stage of Roadmap.
theguardian.com/world/2021/may…
Let me explain why... 1/18

The govt set out 4 tests for proceeding each stage of the roadmap. Tests 1 & 2 relate to vaccination, test 3 is hospitals in no danger of being overwhelmed and test 4 is that there are no new variant concerns.
Test 1-3 have been (easily) met, but I don't think Test 4 has. 2/18
Test 1-3 have been (easily) met, but I don't think Test 4 has. 2/18

Last Friday, Public Health England designated B.1.617.2 (an "Indian" variant) as a variant of concern because of worries that it was more transmissible than B.1.1.7 ("Kent") and cos we didn't know much about its response to vaccines.
What has happened since? 3/18
What has happened since? 3/18
Yesterday new modelling from SAGE SPI-M was released. While they showed that risks of stage 3 of roadmap was much lower with current Kent variant (given high efficacy of vaccines), those risks could *return* for a new variant.
assets.publishing.service.gov.uk/government/upl… 4/18
assets.publishing.service.gov.uk/government/upl… 4/18
In particular, Warwick model (link above) estimated that moving to step 3 of the roadmap risks hsopitals being overwhelmed as in January for a variant just as susceptible to the vaccines *but* 50% more transmissible than our dominant "Kent" variant. 5/18

Having some vaccine escape (even if still protective for severe disease) can also lead to damaging new surges.
SAGE SPI-M emphasise the importance of stopping the spread of any such variant.
gov.uk/government/pub… 6/18
SAGE SPI-M emphasise the importance of stopping the spread of any such variant.
gov.uk/government/pub… 6/18

There have been some estimates that B.1.617.2 is up to 60% more transmissible than Kent (B117)
Admittedly these are based on not great international sequencing data - but it is all we have to go on + we know that much of S Asia in a dire situation.
Admittedly these are based on not great international sequencing data - but it is all we have to go on + we know that much of S Asia in a dire situation.
https://twitter.com/TWenseleers/status/1392457256801816580?s=207/18
The UK Covid genomics consortium (COG UK) released latest data today. It includes sequenced cases from travellers to UK & surge testing, some duplicates & about half of community cases.
Week to 1 May in England, there were 678 cases compared to 365 prev week - almost double 8/18
Week to 1 May in England, there were 678 cases compared to 365 prev week - almost double 8/18
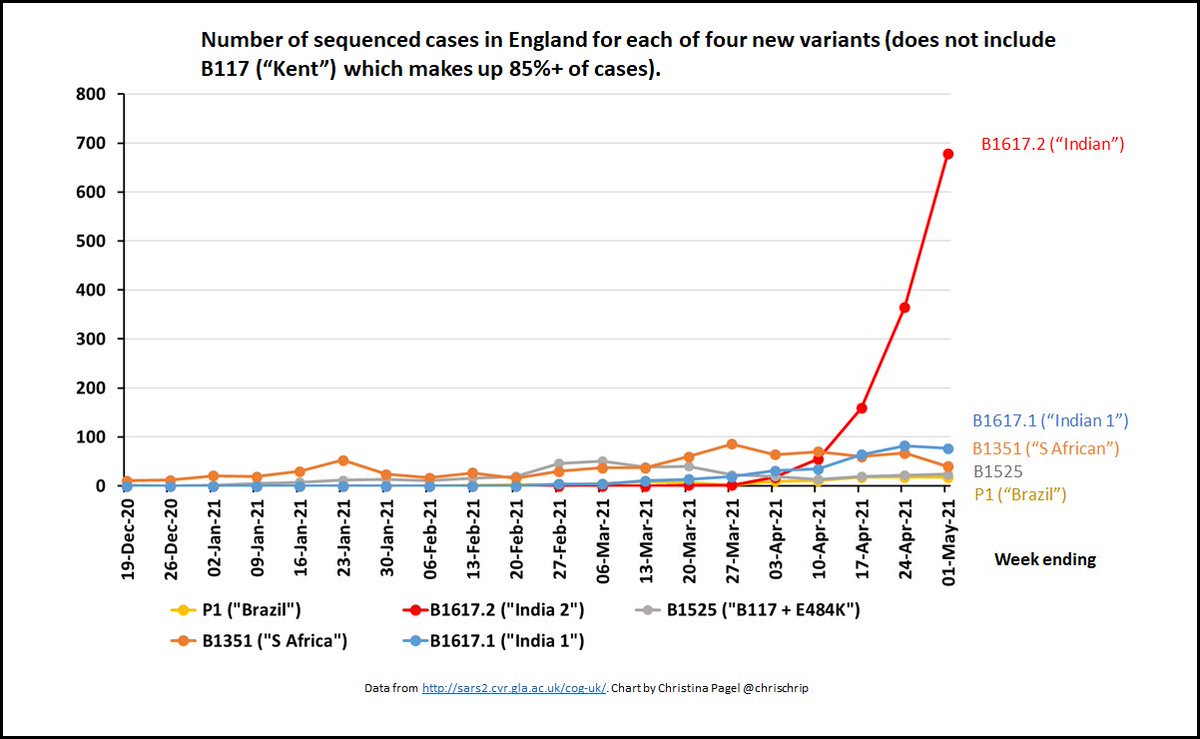
Proportionally, B.1.617.2 was 14% of sequences cases in England. The incomplete data since 1 May is showing the same trend continuing.
In the last week B.1.617.2 was 4% cases in Scotland and 2% in Wales. (No data on NI). 9/18
In the last week B.1.617.2 was 4% cases in Scotland and 2% in Wales. (No data on NI). 9/18

The Sanger Institute takes COG UK data and removed traveller and surge testing data to try to get at what is happening in community. This removes c. half of cases of B.1.617.2.
But exactly the same pattern persists - over 10% of cases in England are B.1.617.2 w/e 1 May. 10/18
But exactly the same pattern persists - over 10% of cases in England are B.1.617.2 w/e 1 May. 10/18

Regionally in England these are concentrated in NW, London and East of England.
Daily average cases in England overall have started consistently going up over the past week as well. 11/18
Daily average cases in England overall have started consistently going up over the past week as well. 11/18

In areas where B.1.617.2 is most concentrated, cases are going up particularly rapidly - e.g. below is Bolton where in most recent week B.1.617.2 was almost 70% of cases.
https://twitter.com/julesmchamish/status/1392499687517720591?s=20(HT to @dgurdasani1 for highlighing this chart) 12/18
So England growth is entirely consistent with increased transmissibility & a situation where B.1.617.2 is rapidly gaining dominance.
We don't yet know enough about vax & B.1.617.2 but there are reports now of some breakthrough symptomatic cases
channelnewsasia.com/news/singapore… 13/18
We don't yet know enough about vax & B.1.617.2 but there are reports now of some breakthrough symptomatic cases
channelnewsasia.com/news/singapore… 13/18
And @GuptaR_lab was quoted in Byline Times today suggesting a delay to the roadmap over concerns about vaccine effectiveness - he stressed that we need to learn more.
bylinetimes.com/2021/05/12/cov… 14/18
bylinetimes.com/2021/05/12/cov… 14/18

Meanwhile, same Warwick SAGE model estimated that if we stayed at stage 2 of roadmap (i.e now) any summer surge would be *much* lower (max ~200 hospital admissions a day instead of over 4000).
SAGE also emphasised that the more people are vaccinated, the lower any surge. 15/18
SAGE also emphasised that the more people are vaccinated, the lower any surge. 15/18

To me, this means that the assessment of the risks IS fundamentally changed by new variants of concern - and so test 4 is failed.
I think we need to either be sure that B.1.617.2 is not a threat OR stamp it out while (if) we still can & vax more quickly. 16/18
I think we need to either be sure that B.1.617.2 is not a threat OR stamp it out while (if) we still can & vax more quickly. 16/18
This means much stronger contact tracing and supported isolation, wider list of symptoms for PCR tests, support for local communities in tackling outbreaks inc maximising vax uptake there.
I also think moving to stage 3 of roadmap right now risks adding fuel to the fire. 17/18
I also think moving to stage 3 of roadmap right now risks adding fuel to the fire. 17/18
Personally, I would like to slow down now to reduce chance of reversing the map later risking more uncertainty, more damaging closures and longer recovery from a worse situation.
We need to learn from previous experience. 18/18
We need to learn from previous experience. 18/18

• • •
Missing some Tweet in this thread? You can try to
force a refresh






















