
Short thread on today's PHE Surveillance Report, covers 3rd-9th May.🧵
Shows very similar case rates to previous weeks, but with some clear divergence for 10-19y/os, and for parts of East mids, NW, and Yorkshire/Humber.
gov.uk/government/sta…
Shows very similar case rates to previous weeks, but with some clear divergence for 10-19y/os, and for parts of East mids, NW, and Yorkshire/Humber.
gov.uk/government/sta…

Furthermore, the significant increases in case rates in some parts of the country continues to raise concerns about potential community spread of variants of concern such as VOC-21APR-02 (first identified in India) among the very places already most impacted by the pandemic.

In the most recent week, case rates in Bolton have doubled from 85 per 100,000 to 188 per 100,000, for Blackburn with Darwen they've doubled to 107/100,000.
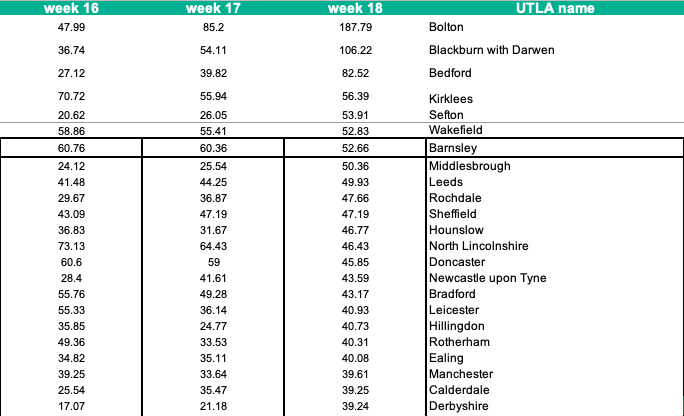
Along with other parts of NW and Mids, these are the very places that have borne the brunt of the pandemic over the past 15 months - both direct harms from infections and deaths, and indirect impacts of lockdown on jobs and livelihoods.

Without addressing the underlying drivers of inequalities such as insecure work and poor housing that fuel viral spread, it won't be possible to truly tackle the virus and realise a genuinely inclusive socioeconomic recovery.
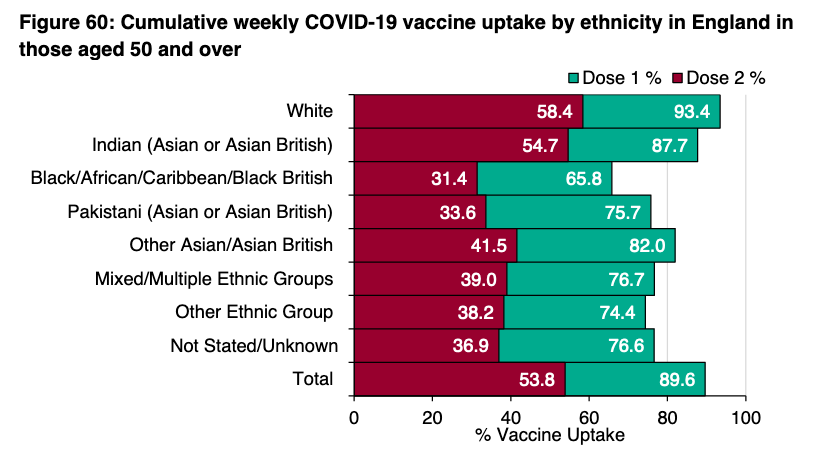
And finally, partly driving these differences is the disproportionate impact of COVID among minority ethnic groups, which in parts of NW and elsewhere is again becoming apparent.

This is related to deprivation, multiple occupancy & multigen housing, and job insecurity - and also overlaps with differential vaccination uptake.
It yet again highlights the critical role of addressing structural inequalities.
jech.bmj.com/content/early/…
thelancet.com/journals/lance…
It yet again highlights the critical role of addressing structural inequalities.
jech.bmj.com/content/early/…
thelancet.com/journals/lance…
PHE surveil rpt👆@felly500 @deb_cohen @martinmckee
@carolecadwalla @mgtmccartney @ADPHUK @Jeanelleuk @fascinatorfun @profchrisham @petermbenglish @HPIAndyCowper @Davewwest
@HSJEditor @KateAlvanley @IndependentSage @nedwards_1 @SamanthaJonesUK @ewanbirney
@FurberA @Dr_D_Robertson
@carolecadwalla @mgtmccartney @ADPHUK @Jeanelleuk @fascinatorfun @profchrisham @petermbenglish @HPIAndyCowper @Davewwest
@HSJEditor @KateAlvanley @IndependentSage @nedwards_1 @SamanthaJonesUK @ewanbirney
@FurberA @Dr_D_Robertson
• • •
Missing some Tweet in this thread? You can try to
force a refresh
























