
This week's T&T data - covers 29/4-05/05
🧵tl,dr:
- fewer LFDs
- fewer cases
- fewer contacts reached and it's taking longer, plus what might be the role of international cases
- and why this is the last update to our @HealthFdn performance tracker.
gov.uk/government/pub…
🧵tl,dr:
- fewer LFDs
- fewer cases
- fewer contacts reached and it's taking longer, plus what might be the role of international cases
- and why this is the last update to our @HealthFdn performance tracker.
gov.uk/government/pub…

Firstly on the TT data.
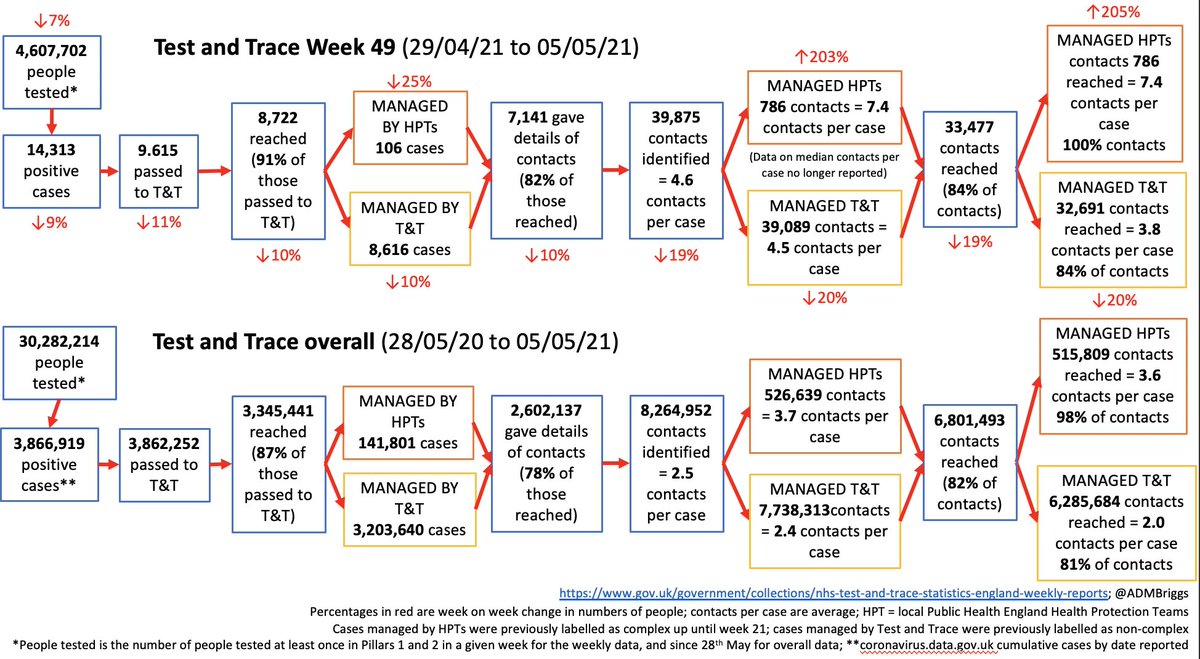
Number of people tested is down this week by 7% to 4.61m, with number of positive cases also down 9% to 14,313.
Number of people tested is down this week by 7% to 4.61m, with number of positive cases also down 9% to 14,313.

The drop in people tested is again due to changes in the use of rapid LFD tests for people without symptoms, rather than changes to PCR test use.
And nearly 2/3 of the fall is due to less reported secondary school testing.
And nearly 2/3 of the fall is due to less reported secondary school testing.

Across the regions, there are ongoing differences in testing rates - lowest in London and the highest in the East Mids.

When looking by local authority, it varies by nearly five-fold.
This could be for very good reasons, but also it may also indicate structural differences in test access with implications for viral spread.
We plan to explore this separately in the coming weeks.
This could be for very good reasons, but also it may also indicate structural differences in test access with implications for viral spread.
We plan to explore this separately in the coming weeks.

Much of the contact tracing performance is largely unchanged.
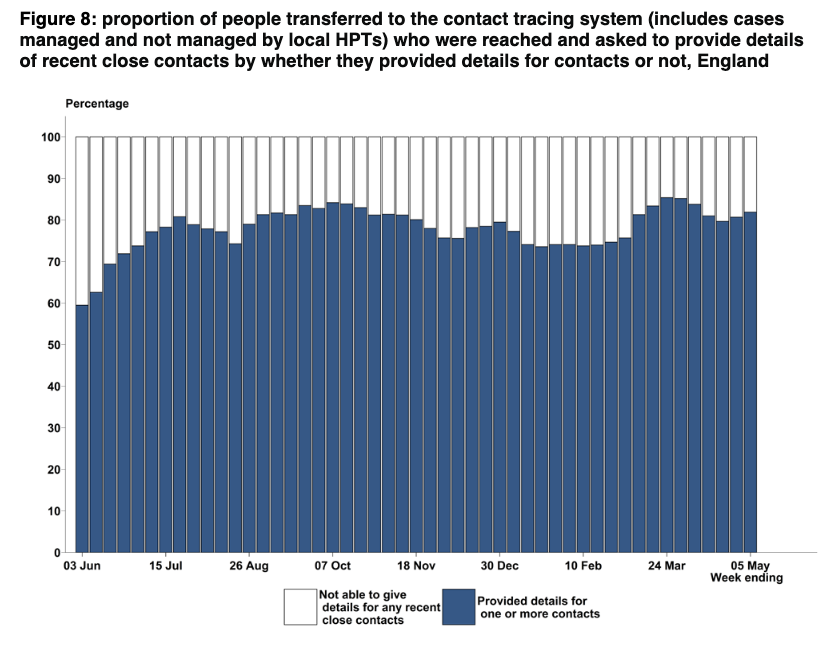
91% of cases were reached, and 82% provided contact details.
39,875 contacts identified with around 4.6 contacts per case.
91% of cases were reached, and 82% provided contact details.
39,875 contacts identified with around 4.6 contacts per case.


But the percentage of contacts reached is falling - now at 84%. Why?

Main reason is that fewer contacts are from the same household as the case. Now just 46%.

Non-HH contacts are more difficult to reach.
The percentage of contacts in the same HH is the same as ever at 96%, and the percentage of non-HH contacts reached is also largely unchanged.
This week it's down a little at 73% compared with generally hovering between 75% and 78%.
The percentage of contacts in the same HH is the same as ever at 96%, and the percentage of non-HH contacts reached is also largely unchanged.
This week it's down a little at 73% compared with generally hovering between 75% and 78%.
One thing mentioned in the T&T report is the impact of international arrivals on contact tracing, and numbers by country are now reported in the data tables.
In the 2 wks from 22/4-5/5, over 800 international arrivals tested positive. In the preceding 2 weeks it was over 1,400.
In the 2 wks from 22/4-5/5, over 800 international arrivals tested positive. In the preceding 2 weeks it was over 1,400.
Here, contact tracing everyone on an aircraft is both arduous and time consuming.
This is seen in the end-to-end times, where % of contacts reached <3 days of the case tested fell from 80% at the end March to 59% 2wks later, before picking up a bit to 68% in the most recent wk.
This is seen in the end-to-end times, where % of contacts reached <3 days of the case tested fell from 80% at the end March to 59% 2wks later, before picking up a bit to 68% in the most recent wk.

And, as mentioned in thread on today's surveillance report, I'm really concerned that yet *again*, its the areas of the country most in need of socioeconomic recovery that are being most impacted by rising case rates and variants.
https://twitter.com/ADMBriggs/status/1392888082454749189?s=20


See @kallmemeg's excellent thread on the latest variant data from earlier this evening for more.
https://twitter.com/kallmemeg/status/1392938581736443910?s=20
And finally, after nearly a year since T&T launched, today's the last (planned) update to our @HealthFdn T&T performance tracker from @cfraserepi and me (big thanks to comms colleagues on this).
health.org.uk/news-and-comme…
health.org.uk/news-and-comme…
As we get closer to it's anniversary, we'll write a short blog about the first 12 months of T&T, but here are some of my thoughts on the situation and why now seems like a good time to stop.


wk 49 T&T☝️ @felly500 @deb_cohen @martinmckee @carolecadwalla @mgtmccartney @ADPHUK @Jeanelleuk @fascinatorfun @profchrisham @petermbenglish @HPIAndyCowper @Davewwest
@HSJEditor @KateAlvanley @IndependentSage @nedwards_1 @chrischirp @SamanthaJonesUK @ewanbirney @devisridhar
@HSJEditor @KateAlvanley @IndependentSage @nedwards_1 @chrischirp @SamanthaJonesUK @ewanbirney @devisridhar
• • •
Missing some Tweet in this thread? You can try to
force a refresh
























