
1/ Report analysis:
Adolescent Boys vs Girls during the Pandemic
A new article is out comparing Suicide Attempt frequency (12-18y) in Catalonia during the pandemic.
It's a succinct article that presents data from the population-level registry that was in place prior to COVID.
Adolescent Boys vs Girls during the Pandemic
A new article is out comparing Suicide Attempt frequency (12-18y) in Catalonia during the pandemic.
It's a succinct article that presents data from the population-level registry that was in place prior to COVID.
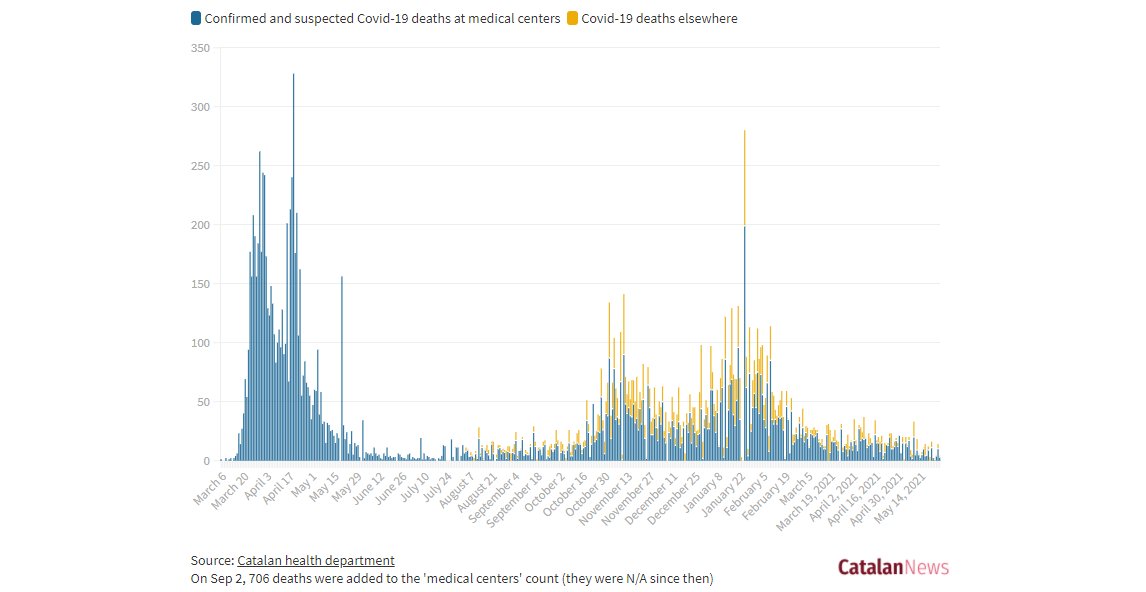
2/ Unfortunately (I really wish they would not do this), it only compares one pre-pandemic year to 2020-21, but this is also a very interesting study because, famously, Catalonia had a devastating early first wave, significant lockdown, then reopening of schools.
3/ What did they do?
They used the CSRC (a database of suicide attempts estbalished in a suicide prevention effort) to look at # of attempts in the year prior to, and the first year of, the pandemic.
They used the CSRC (a database of suicide attempts estbalished in a suicide prevention effort) to look at # of attempts in the year prior to, and the first year of, the pandemic.
4/ What did they find?
For Boys: No significant change for suicide attempts. During both the initial lockdown period AND when schools opened in September, the rates of SAs virtually mirror the rates in the year prior to the pandemic.
Overall -5% compared to the year prior
For Boys: No significant change for suicide attempts. During both the initial lockdown period AND when schools opened in September, the rates of SAs virtually mirror the rates in the year prior to the pandemic.
Overall -5% compared to the year prior

5/ For Girls: a very strong effect was found, in the initial severe lockdown period (Mar-Jun) it followed closely,, but after this (July onwards) there was a steady increase above the previous year. Overall. it was a 39% increase
In the 2nd half: up 73%.
In the 2nd half: up 73%.

6/ Compared to adults in the same database (Down 16.5%), adolescents overall (girls+boys) had an increase of 25%.

7/ It should be noted that in Catalonia kids returned to school in September, so the authors do discuss how combining academic stress + the pressures/changes of the pandemic may have been a factor.
8/ Strengths of the study:
* The surveillance was ongoing - this was not hastily collected post-Covid, so we can compare pre-and-post covid
* It extends right through the first year of the pandemic
* raw subgrouped data in kids! finally!
* The surveillance was ongoing - this was not hastily collected post-Covid, so we can compare pre-and-post covid
* It extends right through the first year of the pandemic
* raw subgrouped data in kids! finally!
9/ Weaknesses:
* 690 suicide attempts were captured, out of ~770k Catalonian adolescents, for a rate of approximately 90/100k, or 0.09%. Adolescents attempt suicide at a MUCH HIGHER rate than this, so there are MAJOR capture issues.
* 690 suicide attempts were captured, out of ~770k Catalonian adolescents, for a rate of approximately 90/100k, or 0.09%. Adolescents attempt suicide at a MUCH HIGHER rate than this, so there are MAJOR capture issues.
10/ This EXTREME undercount (it's estimated that 1-2.5% of all adolescents attempt suicide in any given year by ED capture, and **8% by adolescent survey**). This means that up to 99.8% of all suicide attempts were missed here. This adds a lot of confounders.
11/ * There is significant month-month variability, and even within the year. By only including one pre-pandemic year, the authors may have unintentionally found a spurious result. It's strongly recommended in monthly comparisons to go back at least 3 years from the target year.
12/ * I am NOT a fan of asking a question in the title that is the "significant result." There is more data provided for girls, and it makes me feel that this is post-hoc analysis of a data-set. Fortunately, the difference is so large (P<0.000001), I don't think that matters.
13/ * The girls have far more data than the boys, so it could be that the trend *would* have been seen in boys had more boys been studied. (the ratio of attempts in this study was about 4:1 girls, 2x higher than it should be. Disproportionately, boys were missed)
14/ This is one of the first serious demographic breakdowns of a long enough time period, so it's great to have this data. For whatever reason, the pandemic was harder on girls in Catalonia vs the boys.
15/ To the politically motivated, this cannot be interpreted anything other than "in the year of the pandemic...".
As with all research of this type, it is correlational, and precisely zero cause can be drawn from it.
As with all research of this type, it is correlational, and precisely zero cause can be drawn from it.
16/ There are literally thousands of confounders in a data set like this.
17/ To the ghoulish (using suicide data to make your "should school be open" argument):
* The strongest occurred when schools were reopened (sept+) BUT there were major changes to school (cohorts, mixed online, few sports, etc)
DO NOT USE THIS DATA IN YOUR SCHOOL ADVOCACY
* The strongest occurred when schools were reopened (sept+) BUT there were major changes to school (cohorts, mixed online, few sports, etc)
DO NOT USE THIS DATA IN YOUR SCHOOL ADVOCACY
18/ My conclusions:
* data capture issues
* there was a difference b/w adults (SAs down 16%) and adolescents (SAs up 25%)
* subgroup of girls significant - boys did not have an increase (but not down like adults)
* correlational, no cause can be drawn (if you do, stop it, ghoul!)
* data capture issues
* there was a difference b/w adults (SAs down 16%) and adolescents (SAs up 25%)
* subgroup of girls significant - boys did not have an increase (but not down like adults)
* correlational, no cause can be drawn (if you do, stop it, ghoul!)
19/ The article posits that because girls are more likely to be internalizers, the internalizing symptom increase (anxiety + depressive symptoms) during the pandemic may have disproportionately affected girls. Not sure how I feel about that idea.
20/ We have not seen similar demographics in North America as of yet, from the limited data we have. It does appear that the highest risk period for MH emergency presentations in adolescents is when things are *reopening* on top of pandemic, economic, and social stressors.
21/ The paper is here, but it is behind a paywall. Hence the rough excel tables.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…
• • •
Missing some Tweet in this thread? You can try to
force a refresh




