
1/ There are now about 20 randomized clinical trials (RCTs) of ivermectin for covid. They overwhelmingly show reductions in mortality, when used in adequate doses and in patients who are in early enough stages of the disease.
2 / The Kory et al review encompasses both observational and RCT data. It was published in early May in a peer-reviewed journal, the American Journal of Therapeutics, and is already the most-viewed paper in the journal’s history. It's also very readable.
journals.lww.com/americantherap…
journals.lww.com/americantherap…
3 / The Bryant, Lawrie et al metanalysis is very rigorous (only considers the RCTs etc) and reaches similar conclusions: about a 70% relative reduction in mortality when used in adequate doses and early enough. (Lawrie is a veteran Cochrane reviewer.)
https:2.1//osf.io/k37ft/
https:2.1//osf.io/k37ft/
4/ Now some reminders. A randomized clinical trial (RCT) assigns randomly a share (typically half) of the patients to a group that receives the treatment, and the remainder are assigned to a group (the “control group”) that does *not* get the treatment.
5/ The difference in a given outcome (for example death) between the 2 groups is the estimate of the effect of the treatment. If 4% of the treatment group and 12% of the control group died, then the "relative reduction effect" was 67%, meaning the % of death was reduced by 2/3
6 / Small RCTs have small samples and are subject to plenty of statistical “noise” (i.e., “good or bad luck”). Organizing very large RCTs is expensive and cumbersome. Only large pharma companies and state bureaucracies can do that. For cheap generic drugs this very rarely happens
7/ With only small or medium-size RCTs one does a “metanalysis”. A metanalysis pools the data from several smaller RCTs, then analyses them jointly to obtain more precise estimates of both the *size* of the effect and of the *probability* that it actually exists.
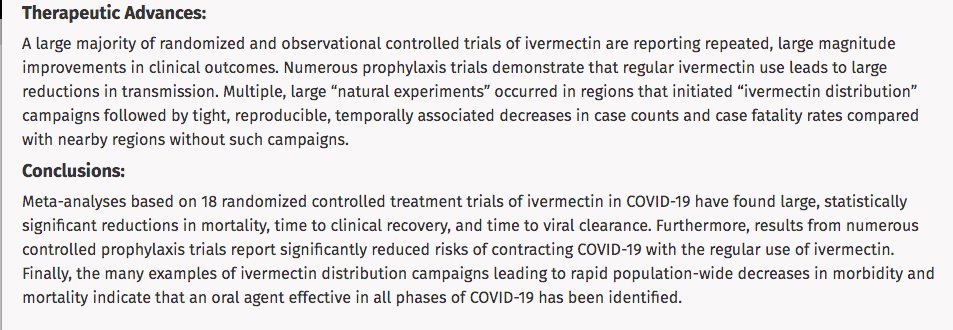
8/ In a metanalysis the “forest plot" shows the estimates of each RCT and of the pooled analysis. (In the screenshot: effect on death from the Bryant-Lawrie metanalysis.)
9/ Diamonds to the left of the vertical line show that the ivermectin group did better than the control group in that RCT. The bottom diamond is the joint, pooled result of all the RCTs.
10/ All of the RCTs above show reductions in death, with two exceptions: Rezai, a tiny RCT (so with a lot of room for luck, good or bad) with 1 death in IVM group and 0 deaths in control; and Fonseca/Galan, an RCT in severe hospitalized patients where the groups essentially tied.
11/ The pooled estimate of the Bryant-Lawrie metanalysis is an 72% relative reduction in deaths. Kory at al reaches a similar estimates. So does the data from every comprehensive metanalysis of ivermectin for covid in early treatment.
12/ Now for *safety* of ivermectin: it is extremely safe in adequate doses. The pre-covid (therefore pre-politization) literature tested safety with doses even 10x the doses typically used for covid, see for instance the linked paper
ascpt.onlinelibrary.wiley.com/doi/full/10.10…
ascpt.onlinelibrary.wiley.com/doi/full/10.10…
13/ Also regarding safety, Merck has donated more than 4 billion [sic] doses to Africa and other countries. (More on Merck and ivermectin further down the thread).
mectizan.org/partners/merck/
mectizan.org/partners/merck/
14/ Now for a few caveats. First, it’s not clear how much or whether ivermcetin is effective in *severe* hospitalized patients. The Fonseca/Galan et al RCT is fairly small but suggests it might not be effective in that very advanced stage: tandfonline.com/doi/full/10.10…
15/ Second caveat: some advocates have overreached in claiming that ivermectin will “end the pandemic”. The RCT data show it won’t, but will reduce GREATLY the number of deaths (as it is currently doing in Mexico city, parts of India and a growing number of regions and countries)
16/ Third caveat: even if the true mortality efficacy of ivermectin for early covid is actually close to the 70% relative reduction found in the metanalyses above is correct, this is still well below the mortality reduction of the main vaccines.
17/ Choosing BETWEEN early treatment and vaccines is a false dichotomy. BOTH should be used, given good safety profiles. Lots of people who don’t have access to vaccines yet. This includes as of now most people in my country, Brazil, where about 2000 people are dying each day.
18/ Treatment is for those with covid; vaccines are for the broad population (with priority for at-risk groups). The tribal dispute between treatment proponents and vaccination proponents is one of the most irrational and destructive tribalisms humanity has ever witnessed.
19/ Ivermectin has both antiviral and antinflammatory properties. This makes it specially suited for covid in early phases of disease.
Here Eli Schwartz of Tel Aviv University explains the antiviral properties found in his RCT:
Here Eli Schwartz of Tel Aviv University explains the antiviral properties found in his RCT:
20/ Roughly speaking, the “p-value” of an RCT gives the certainty of the effect found in a given RCT. An RCT where the ivermectin group does better than the control group with p-value > 0.05 is NOT evidence *against* efficacy, but instead (weak, by itself) evidence *for* it.
21/ Lots of weak evidence constitutes strong evidence; this is what the ivermectin metanalyses show. The effect is often so strong that p<0.05 is attained even in isolated small RCTs. Jointl, the RCTs yield very strong evidence of efficacy (when early, adequate doses etc)
22/ This Nature paper explains among other things the basic “bright-line fallacy” of mistaking weak evidence for efficacy for (strong) evidence against efficacy:
nature.com/articles/d4158…
nature.com/articles/d4158…
23/ Another point: “preprints don’t count” is science-as-bureaucracy, a lawyer’s argument. Data, duly parsed, speaks. The ivermectin RCT data speaks volumes: there were large, consistent reductions in mortality in the early treatment and moderate hospitalized RCTs.
24/ In any case, there are several of peer-reviewed RCTs by now. The Mahmud, Okumus, and Chaccour RCTs are already published at this point. The Lopez-Medina RCT published in JAMA had 0 deaths in IVM group and one in control group (also less clinical deterioration etc). And so on.
25/ By the way, the Bryant-Lawrie metanalysis (item 3 in this thread) has been accepted for publication in a peer-reviewed journal. The Kory et al review (item 2) is already published. Others are forthcoming.
26/ Arguing for the blanket exclusion of the RCTs as “low quality” is a copout. For a “hard”, unambiguous outcome such as death, only massive, coordinated fraud across continents by the researchers running these RCTs would explain these results.
27/ Here is a video interview of Lawrie (of the Bryant-Lawrie metanalysis) addressing these and other issues:
28/ In addition to all the (human) RCTs, there is also an "animal model" study on mice published in Nature Scientific Communications indicating efficacy (in an animal study the subjects can be autopsied, yielding finer data on organ damage and so on):
nature.com/articles/s4159…
nature.com/articles/s4159…
29/ In 2015 Satoshi Omura won the Nobel Prize in Medicine for having among other things discovered ivermectin. In the paper below Omura et al argue and give a rationale for the mass use of ivermectin for covid:
jja-contents.wdc-jp.com/pdf/JJA74/74-1…
jja-contents.wdc-jp.com/pdf/JJA74/74-1…
30/ Now for the notorious Merck note arguing that there is no effectiveness or safety data for ivermectin. On safety, Merck has donated > 1 billon doses. On effectiveness, see this whole thread.
31/ Ivermectin is cheap, abundant, and under no patent. Monulpiravir, on the other hand, is the (expensive, patented) antiviral that Merck is marketing. Do the math.
32/ If you doubt the capacity and willingness of large drug companies to misinform the public, read up on Merck’s disinformation campaign on Vioxx:
i. newscientist.com/article/dn1368…
ii. nbcnews.com/health/health-…
i. newscientist.com/article/dn1368…
ii. nbcnews.com/health/health-…
33/ Now some observational data. The Mexico city government recently did a citywide test on early patients, comparing those who took and didn't take ivermectin. The results are explained (in Spanish
facebook.com/GobiernoCDMX/v…
facebook.com/GobiernoCDMX/v…
34/ After the test above the Mexico city government decided to systematically use ivermectin for early covid (efe.com/efe/usa/mexico…). So have parts of India and a growing number of other regions and countries.
35/ State bureaucracies and agencies are usually slow and often incompetent (remember the WHO recommendation *against* masks until June 2020?) . Regulatory capture by industry is a problem. As is sheer incompetence: see for example the "bright-line fallacy" in items 20 to 22.
ARGH! Here's the correct link to the Bryant-Lawrie metanalysis: osf.io/k37ft/
36/ With all this, why the fierce opposition to early treatment? The mantra “there is no such thing as early treatment” is to covid treatment just as “the lab leak hypothesis is a conspiracy theory” is to covid origins. It is unambiguously false.
37/ Several other early treatments with cheap repurposed drugs have with solid evidence of efficacy, including fluvoxamine (one RCT in JAMA, an upcoming larger RCT with postive preliminary data) and inhaled budesonide (two Oxford University RCTs, STOIC and PRINCIPLE)
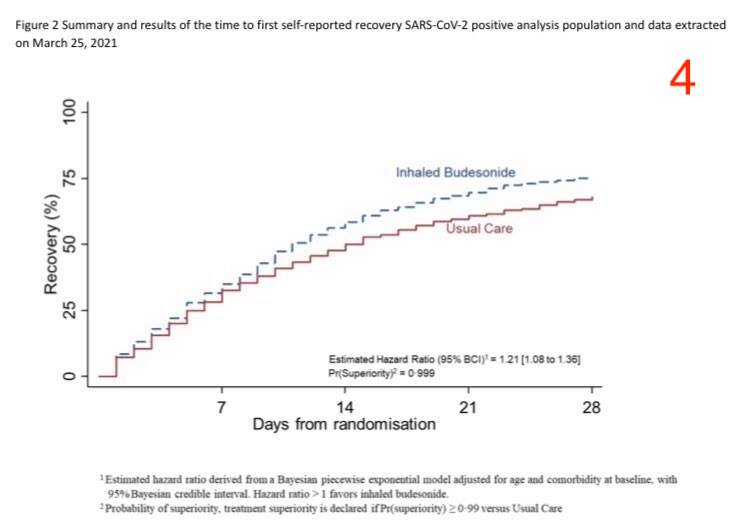
38/ By the way, after the STOIC RCT -- published in Lancet Respiratory Medicine -- and the PRINCIPLE data (see the Kaplan-Meyer curve in screenshot #4) even the UK’s uber-conservative NHS has authorized its use in at-risk outpatients:
england.nhs.uk/coronavirus/wp…
england.nhs.uk/coronavirus/wp…

39/ The groupthink against early treatment comes from a perfect storm: politicization, regulatory capture, statistical incompetence, bureaucratic mindset, reflexive deference to authority. In all this, the early treatment taboo resembles the (former) lab leak hypothesis taboo.
40/ Sometimes condescension+paternalism play a role. In the words of an academic acquaintance: “Imagine if it becomes mainstream that [early treatment] is effective (…) sometimes you have to manipulate information given [the public’s cognitive] constraints. Food for thought.”
41/ The groupthink has led to the active suppression of information. “Fact checkers” have banned posts and tweets on RCT data just as they used until recently to do to lab leak texts. The fact-checking is generally ignorant, biased and very often plain incorrect (oh, the irony).
* in Spanish, starting in minute 16
* 1 billion doses
42/ I’ve been a target myself. Some of my posts (in another social network) on the subject have been cancelled and my account temporarily locked out. A journalist [sic] asked Twitter to ban a thread discussing and linking to early treatment RCTs. Strange times.
* only considers the RCTs for mortality
* Kaplan-Meier
43.a/ BEGINNING OF UPDATED THREAD (03/08/2021): below follow updates incorporating new data, including the retraction of the Elgazzar RCT
43.b/ The tl;dr of the updates:
i. the evidence for strong efficacy of ivermectin treatment of severe patients, which was already mixed (see item 14 of thread), has been further weakened
i. the evidence for strong efficacy of ivermectin treatment of severe patients, which was already mixed (see item 14 of thread), has been further weakened
43.c/ The tl;dr of the updates:
ii. There is more noise in the early treatment RCT data. The bulk of the RCT data point to substantial efficacy, but even at optimal timing and dosage *ivermectin is neither a silver bullet nor nearly effective as vaccines* (see items 16 and 17).
ii. There is more noise in the early treatment RCT data. The bulk of the RCT data point to substantial efficacy, but even at optimal timing and dosage *ivermectin is neither a silver bullet nor nearly effective as vaccines* (see items 16 and 17).
43.d/ The tl;dr of the updates:
iii. This thread is concerned with ivermectin for treatment, not prophylaxis. Given that ivermectin is not a silver bullet for treatment, it's unlikely to be a silver bullet for prophylaxis either. See this discussion:
iii. This thread is concerned with ivermectin for treatment, not prophylaxis. Given that ivermectin is not a silver bullet for treatment, it's unlikely to be a silver bullet for prophylaxis either. See this discussion:
https://twitter.com/AbdenurFlavio/status/1421527934368636928?s=20
44/ Like so many covid-related topics, much of the discussion on ivermectin has been radicalized. The positions of both the "ivermectin ends the pandemic" and the "ivermectin is for worms" camps are unsupported by current data. The polarization is doing a lot more harm than good.
45/ Including the Vallejos RCT and excluding the Elgazzar RCT in a random effects metanalysis model yields a 62% point estimate for mortality reduction for the early treatment (encompassing both outpatient and early hospitalized) RCTs, with p-value of 7%, see screenshot.

46/ Note also that the same holds for other clinical outcomes of the early treatment RCTs, and that moreover there are two animal model RCTs with clinical benefits published in peer-reviewed journals by Institut Pasteur groups:
embopress.org/doi/full/10.15…
nature.com/articles/s4159…
embopress.org/doi/full/10.15…
nature.com/articles/s4159…
47/ Beware once again the bright-line fallacy. A p-value of 7% with a point estimate of substantial clinical benefits does not constitute evidence *against* efficacy; quite the contrary. See items 20, 21 and 22 of thread.
48/ In sum, the uncertainty around true effect size of early treatment with ivermectin has increased, but the data still lean heavily towards clinical efficacy. It might be a statistical fluke, but that still looks unlikely.
49/ On the other hand, the evidence for substantial mortality reductions in *late* treatment has long been mixed and is now further weakened. And the argument for prophylaxis with ivermectin as a *replacement* for vaccination never held water (see items 15, 16, 17, 18, 43c, 43d).
50/ UPDATED THREAD (22/08/2021): below follow updates incorporating new data on early treatment ivermectin RCTs, now including the Together outpatient trial and further remarks on the overall picture at the moment
51/ The Vallejos RCT (see link) has found mixed results on an early patient cohort: e.g., comparing IVM and placebo groups, there was 35% less hospitalization (14 in IVM vs 21 in placebo) but 1 more death (4 in IVM vs 3 in placebo).
bmcinfectdis.biomedcentral.com/articles/10.11…
bmcinfectdis.biomedcentral.com/articles/10.11…
52/ The Vallejos (a.k.a. IVERCOR) RCT is well-written and points out that it was underpowered and the dosage it used (0.2mg per kg for two days) is lower than the dosages currently recommended as effective. It must be included in metanalyses, including dose-dependency analysis.


53/ Now for the Together trial. With moderate dosing and mean 4 days of symptoms at the start of treatment, it measured a 9% reduction in the risk of clinical deterioration and an 18% reduction in the risk of death, with high p-values.

54/ A Bayesian analysis by the Together authors on their own data yielded a 76% probability of IVM being better than placebo. Weirdly but not surprisingly (the subject has become Rorschach test), some are treating Together as definite evidence that IVM does *not* have an effect.

55/ On the other extreme, some ivermectin enthusiasts are attacking Together as a sham trial -- when it actually looks very much like an honest, well-conducted RCT. Again, tribalism and groupthink created a Rorschach test.
56/ In any case, after the retraction of Elgazzar and the inclusion of Vallejos and Together (a) the mean estimate for efficacy of early treatment with IVM has lowered, and (b) the uncertainty has increased.
57/ About effect size: one estimates effect on mortality by comparing % of death in IVM group with % of death in control group. RCTs on mild-moderate patients have few deaths in both IVM and control groups. . Low #s of deaths —> higher uncertainty regarding the “true” effect size
58/ Here's the updated random effects metanalysis for mortality of the early treatment ivermectin RCTs. Elgazzar has been excluded; Together and Vallejos have been included. The point estimate of relative reduction is at 51% and the p-value at 0.09.

59/ It's still more likely than not that with adequate doses+timing IVM substantially reduces the risk of deterioration+death, but it has become plausible that the mean effect in the RCTs results from a combination of (a) statistical flukes and (b) one or more fraudulent trials
60/ Misinterpretation of data has reinforced polarisation. On one hand some IVM proponents greatly exaggerate its likely effect. On the other hand some on the opposing camp cherry-pick RCTs and stick to the “if p>0.05 then there is no evidence” fallacy (see item 22).
61/ As futher info and more RCT data come in, using different dosages and timings of start of treatment, the picture on the true effect sizes (of various dosages / timings) will become clearer. This is simply how data / science (and indeed outright logic) work.
• • •
Missing some Tweet in this thread? You can try to
force a refresh









