I still see ppl claiming having vaccine side effects or reactions is a sign of the vaccine ‘working’. This is false, please do not cause unnecessary worry to those who did not experience any side effects.
Let me try & explain. /continue
Let me try & explain. /continue
The immune system respond to the vaccine (or any foreign pathogen) by 2 ways.
1. Innate immunity: this is the initial response where all the white cells come out & play, trying to clear the body from the foreign particles. The physical manifestations r fever, body ache etc.
1. Innate immunity: this is the initial response where all the white cells come out & play, trying to clear the body from the foreign particles. The physical manifestations r fever, body ache etc.
The innate immunity response is not a measure of how hard the body is working or building antibodies. And can be addicted by various factors: age, gender, co-morbids, stress, lack of sleep, hormones. List goes on.
2. Adaptive immunity: this is the period when the other part of then immunity, T & B cells learn about the foreign particles & start to prepare antibodies (now & for future reactions).
This immune response has no physical manifestations.
This immune response has no physical manifestations.
Only way to check if the body has developed protection against the foreign particle, SARS-CoV-2 virus in this case, is to check antibody titres.
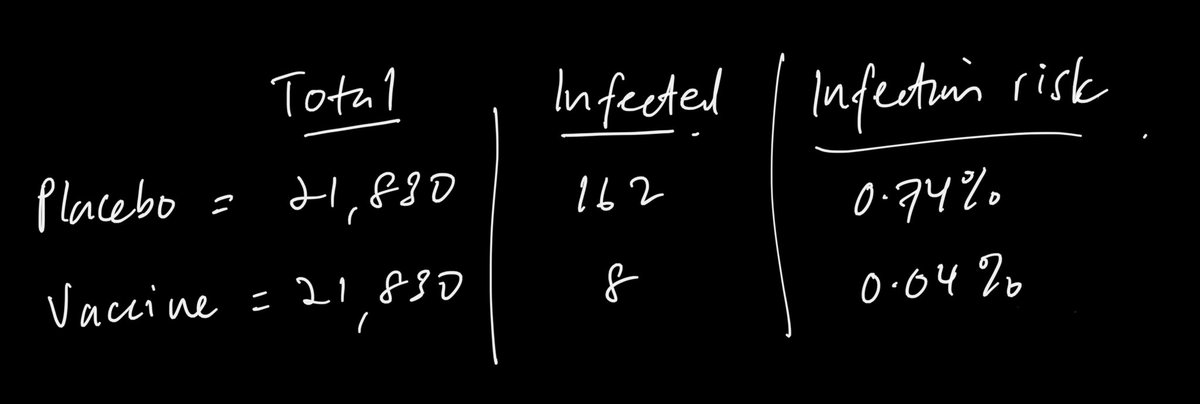
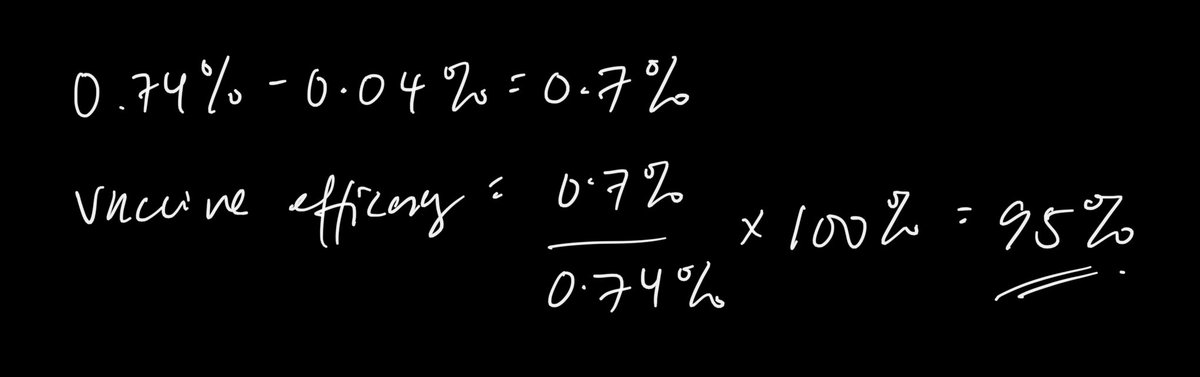
That is why in the Pfizer P3 trials, only ~50% of vaccinated developed s/effects but protection after checking antibody is ~95%.
That is why in the Pfizer P3 trials, only ~50% of vaccinated developed s/effects but protection after checking antibody is ~95%.
*can be affected 🙄
Think of it this way: if u go out for a run, u tripped over a tree root & hurt your knee.
Innate immunity is when u put a bandage on it. U also feel pain when u wash it with antiseptic lotion.
Innate immunity is when u put a bandage on it. U also feel pain when u wash it with antiseptic lotion.
Next time when u run at the same place, your brain remembered that root & u simply hop over it. This is adaptive immunity. U don’t feel anything but avoided the fall.
Ok maybe not best analogy 😂 but remember side effects r not an indication of whether vaccine is working!
Ok maybe not best analogy 😂 but remember side effects r not an indication of whether vaccine is working!
• • •
Missing some Tweet in this thread? You can try to
force a refresh