The Delta variant: updates from the new @PHE_Uk report
assets.publishing.service.gov.uk/government/upl…
1st dose vaccine (either AZ or Pfizer) quite protective vs hospitalization
Fully vaxxed vs unvaxxed:
Infections 7.7% vs 67%
Hospitalizations 8% vs 48%
assets.publishing.service.gov.uk/government/upl…
1st dose vaccine (either AZ or Pfizer) quite protective vs hospitalization
Fully vaxxed vs unvaxxed:
Infections 7.7% vs 67%
Hospitalizations 8% vs 48%

Delta's secondary attack rate is coming down some in the latest dataset. Its enhanced transmission over alpha appears to be more in the 40-60% range
Reinfections by sequencing data: 311/1260 were Delta
Reinfections by sequencing data: 311/1260 were Delta


This 71-page report is rich. And that 60% of infections are getting sequenced (91% are Delta) is quite impressive.
It makes the output from CDC and the genomic surveillance in the US particularly weak
It makes the output from CDC and the genomic surveillance in the US particularly weak
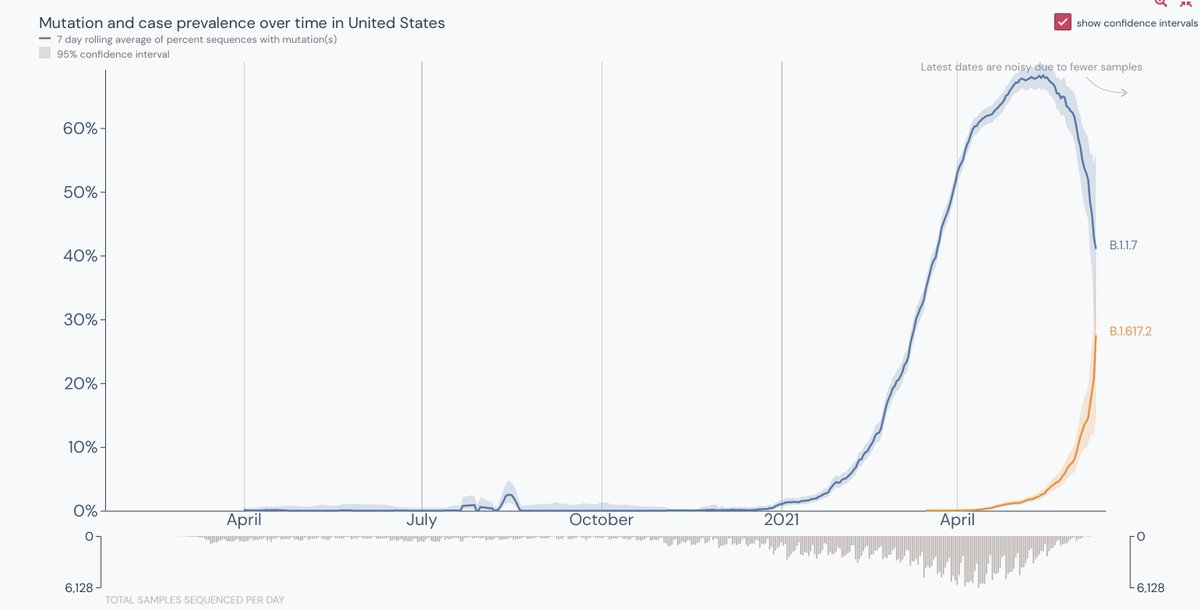
Here is the latest @CDCgov variant report. It is from May 22 and it's frankly pathetic when you compare it to @PHE_UK, both with respect to it being out of date and the lack of sequencing in the US
covid.cdc.gov/covid-data-tra…
covid.cdc.gov/covid-data-tra…

Contrast today's @PHE_UK report from genome sequencing (60% of cases) up to 4 days ago -- >60,000 Delta cases with vaccination status and outcomes


• • •
Missing some Tweet in this thread? You can try to
force a refresh