
A quick Sunday case data round-up. First, the age-group growth rate charts continue to show a declining trend in short-term growth. I’ll start with the 0-30s today: 

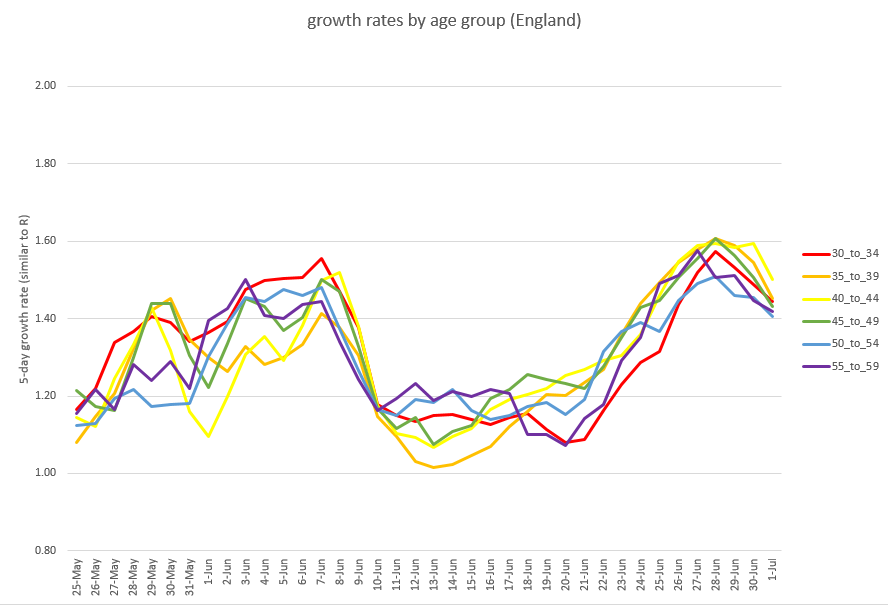
and then the 30-60s, also with a clear declining trend:
and lastly the 60-90s, now mostly holding at a fairly steady growth rate (which is better than where they were a few days ago, with accelerating growth). (ctd)

I think the question is no longer: is growth falling? But rather: what will it do next? Does it keep going down (great news), stabilise at a new level (less good, but still better than it was), or bounce back up (bad news)? Mesdames et messieurs, faites vos jeux….
Taking a quick look at the regional data, it’s clear that (as others have noted, and I flagged as a concern over 2 weeks ago), the North East is now the region with the highest case rates – and still concentrated in the 10-30 year olds:
https://twitter.com/JamesWard73/status/1405602408659623951?s=20

And looking at growth rates rather than case rates, the North East remains in the lead (which is not a good place to be). I’m not particularly liking the trend in the South East either.

Finally, just keeping an eye on the male:female split, in case the football makes a difference. Case rates continue to be more male-biased than normal, and particularly in the 15-40s (and, more surprisingly, the 75-90s). But there’s been no big shifts in recent days. /end

• • •
Missing some Tweet in this thread? You can try to
force a refresh



