
🧵 - on #Obesity #inequalities who they affect most and what can be done about it.
All the findings are in this new @TheKingsFund report, so let's pull out some of the key issues 👀👀
kingsfund.org.uk/publications/t…
All the findings are in this new @TheKingsFund report, so let's pull out some of the key issues 👀👀
kingsfund.org.uk/publications/t…
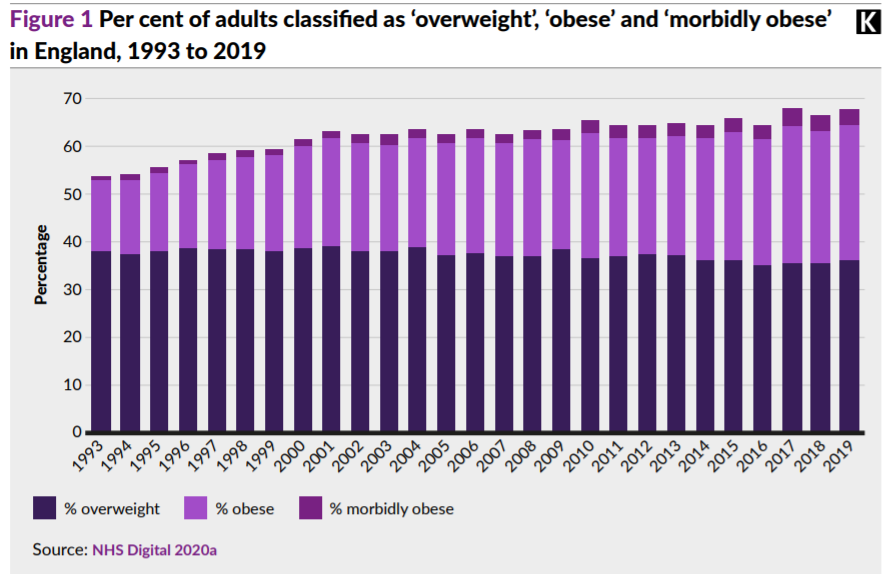
Numbers of people who are obese are⬆️ rising in real and relative terms.
Since early 2000s overall overweight prevalence topped out at ~2/3 of adults, BUT - underlying trend is ⬆️ obese ppl as a proportion of overweight.
Since early 2000s overall overweight prevalence topped out at ~2/3 of adults, BUT - underlying trend is ⬆️ obese ppl as a proportion of overweight.
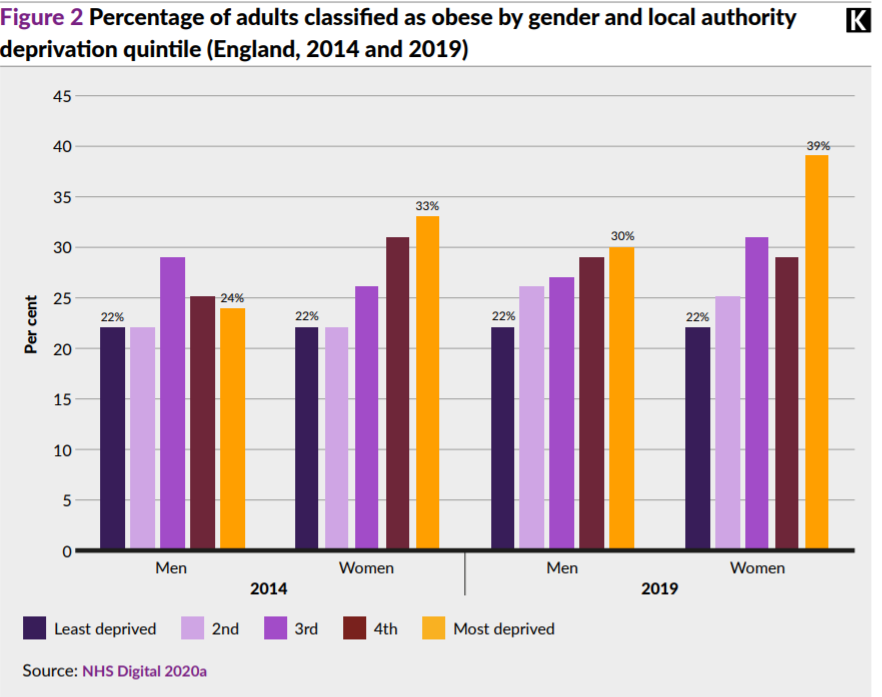
While the national picture is clear, it masks some deep inequalities...
➡️8 point gap in male obesity between most & least deprived.
➡️17 point gap for women.
➡️Women from most deprived experience the very highest rates at 39%.
And... the gap has widened significantly.
➡️8 point gap in male obesity between most & least deprived.
➡️17 point gap for women.
➡️Women from most deprived experience the very highest rates at 39%.
And... the gap has widened significantly.
There's also a really stark geographical spread. The highest rates of obesity are clustered around urban & post industrial areas of North E&W plus the Midlands, or in politico speak "the red wall"...

We know obesity is bad for our health - so the way that these disparities translate to health inequalities is not surprising...
➡️Most deprived communities see obesity admissions 2.4 times that of most affluent.
➡️Most deprived women worst affected, with rates 2x that of men.
➡️Most deprived communities see obesity admissions 2.4 times that of most affluent.
➡️Most deprived women worst affected, with rates 2x that of men.


So, what can be done and does the NHS have a role to play? Yes, of course!
➡️Invest in weight management services.
➡️Train staff in nutrition & to have conversations about diet.
➡️Leverage power as an "anchor institution".
➡️Include it as part health inequalities strategy.
➡️Invest in weight management services.
➡️Train staff in nutrition & to have conversations about diet.
➡️Leverage power as an "anchor institution".
➡️Include it as part health inequalities strategy.
BUT, BUT, BUT... the NHS is not an island. The causes of obesity are social and economic, so prevention requires a broader x-government approach to health.
We've seen how effective use of taxation and regulation can improve health, more of this!
kingsfund.org.uk/publications/t…
We've seen how effective use of taxation and regulation can improve health, more of this!
kingsfund.org.uk/publications/t…
Obesity policy over the last 30 years has been piecemeal and ineffective.
The current obesity strategy risks continuing that tradition, so instead of going down a route we know doesn't work, lets try something a little different...
ENDS
The current obesity strategy risks continuing that tradition, so instead of going down a route we know doesn't work, lets try something a little different...
ENDS
• • •
Missing some Tweet in this thread? You can try to
force a refresh


