
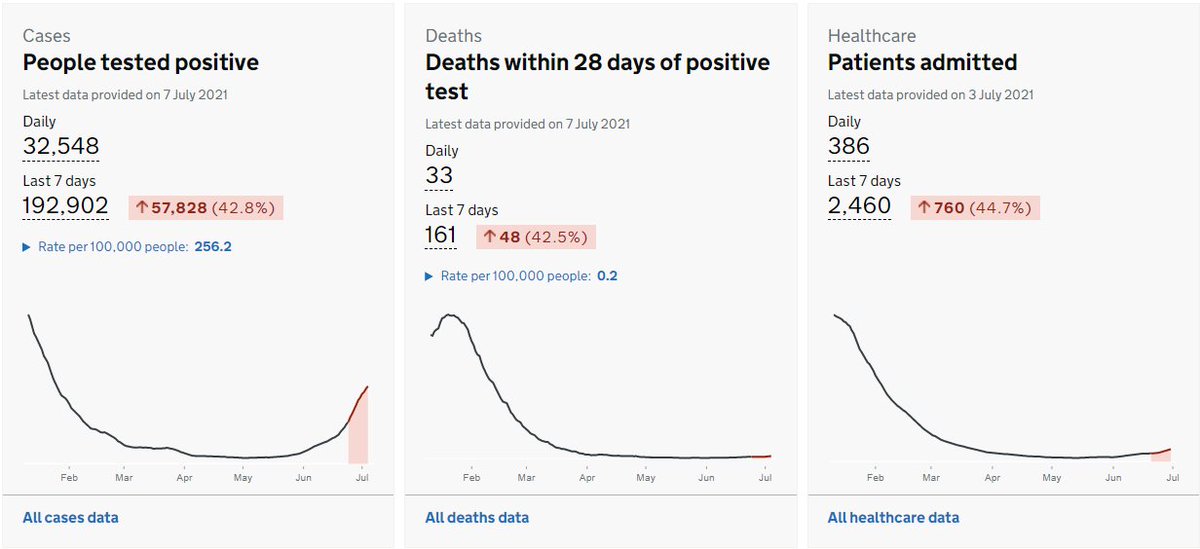
There’s plenty of bad news on the dashboard this evening, with hospitalisations and deaths joining cases in growing by over 40% week-on-week. But is it just me, or does that case curve look like it’s starting to curve over to the right? 
Of course, this will be no surprise to anyone who’s been paying attention to the age-stratified growth rates over the last week. And the pattern here continues, with growth rates continuing to fall in the under-30s:

and in the 30-60s:

However the trend in the 60-90s is less good, with (on average) flat growth levels, still too high (c. 50% over 5 days) – and the growth in this group is now higher than in the under-60s. That’s not good news for the trend in admissions and deaths over the next 2-3 weeks

Also please note that we’re currently seeing high levels of late cases being reported. This means that the last 1-2 days of my graphs might be under-estimating growth. I don’t think it will change the direction, but it might just adjust the slope.
https://twitter.com/chrisdrakeuk/status/1412808795559010305?s=20
If we look at the overall (all ages) growth, there is a clear trend, and it’s possible to get excited: another week or so on that line and we’d be at R=1 (i.e. cases peaking). I think that’s probably too optimistic; the trend looks too strong to be a pure vaccine effect,

… and so there’s probably other factors involved – and there’s also still a lot of variation by age group and by region, all of which makes it hard to call whether growth continues down, finds a new level or bounces back up. But at least it’s going in the right direction. /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh



