
there's probably a meme for this: 

and to put it in context, here are the other age groups: (first 0-30s)

and 30-60s

and 60-90s

so it does look like the rate at which growth is falling is itself falling (is that a positive third derivative? - I'm losing track). and particularly in the young-adult groups (15-35) we may have settled to a new rate - or could even be starting to bounce back to higher growth
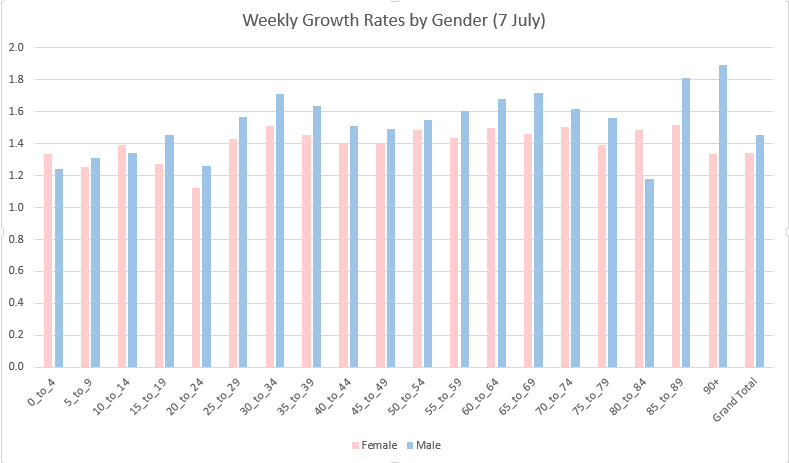
and if you're tempted to blame this on the football... I think you're probably right (at least in part). the timing fits with last weekend's match, and the growth is biased to males over the last week, in nearly every age group.
in a way that's good news: the number of football matches is not increasing exponentially, and so while we might see a "bump" in cases from this, it should fade over the following weeks. 🤞
and in case you're wondering: no my model didn't assume that growth would continue to fall at its previous rate (but it did assume a continued, gentler, fall - so if growth did start growing again that would be an issue)
• • •
Missing some Tweet in this thread? You can try to
force a refresh



