The drop to 44% protection vs sympt dz 5mo after RNA dose2 suggests a rapid drop of circulating antibodies. The immune system does not sustain the high amounts of nAbs needed to block symptomatic infection. Makes sense it would only produce those high levels after the RNA punch. 

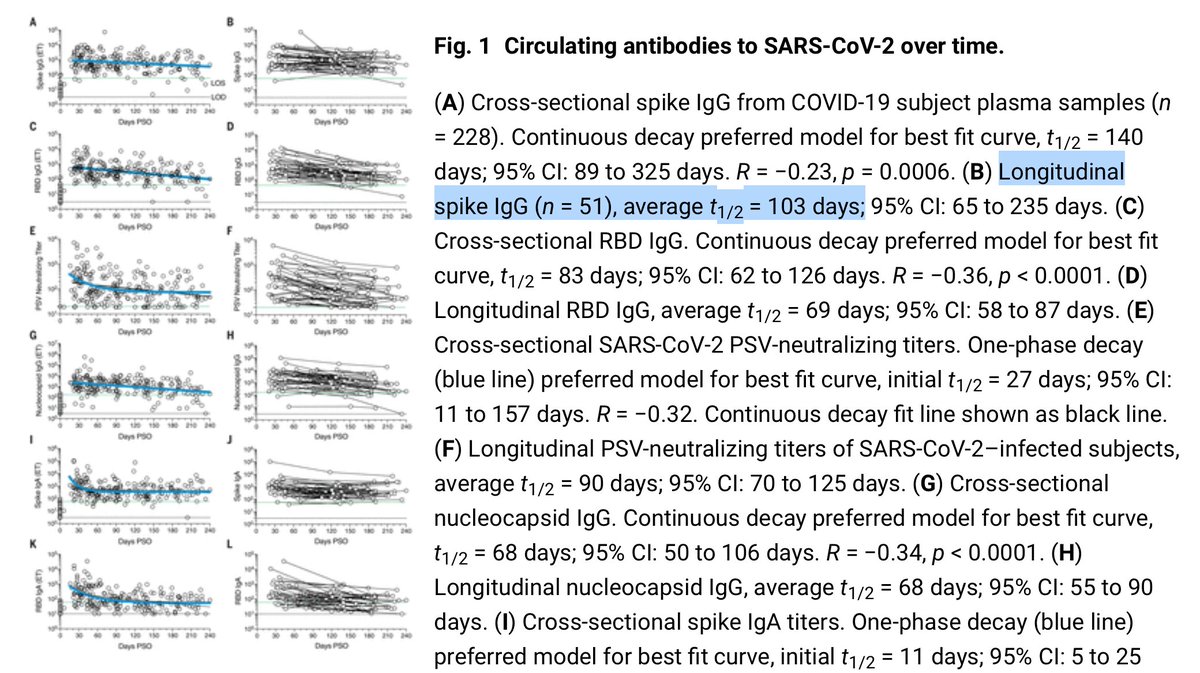
This paper found the half-decay time of anti-SARSCoV2 antibody levels to be 2-3 months after infection.
academic.oup.com/pcm/article/4/…
academic.oup.com/pcm/article/4/…


Another larger study in Science similarly measured half-life of 100 days for antibodies (note log scale)
science.sciencemag.org/content/371/65…
science.sciencemag.org/content/371/65…
There isn't a linear correlation between nAb levels and % symptomatic breakthrough of course. So here we lose 50% of the protection (~88 to 44% breakthrough rate) in 5 months, which corresponds to ~75% reduction in antibody levels.
This is just about your ability to have high enough circulating nAb levels for mucosal immunity: stopping enough virus from entering cells that you don't even have symptoms. So even if your nAb levels have decayed and you get symptoms, the vaccines already gave you a head start
...in that your trained B and T cells are already there and can ramp up activity upon breakthrough to produce more nAbs again and kill infected cells, preventing progression to severe disease.
It also goes without saying that this doesn't mean your long term ability to recognize and fight SARSCoV2 is being lost with 50% probability in 5 months either. You have memory B and T cells that survive for years and can proliferate in response to re-encounters.
So when you hear talk about immunity waning and then the next day talk about how you have lifelong protection, they are not contradictory. Your immune system is designed to react to ongoing challenges with antibody production.
Your circulating levels of Abs wane because you can't possibly keep nAb levels high for every antigen you've ever encountered. But you still have lifelong protection in B and T cells watchfully waiting.
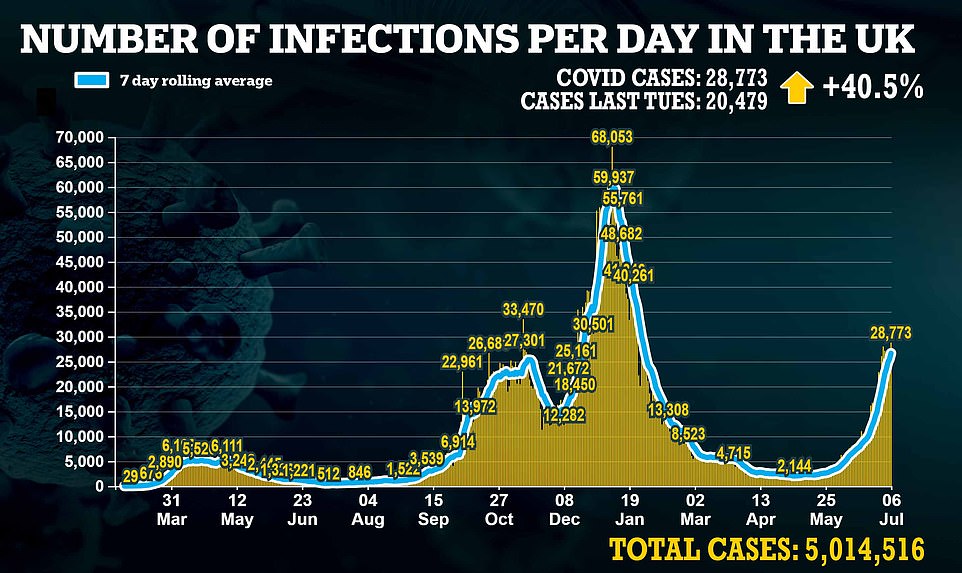
This does mean that to protect against symptomatic disease which is also transmissible disease, we would need boosters every 6 months. If nearly everyone worldwide were immunized synchronously then we could reach herd immunity, i.e. the virus stops propagating.
However it seems unlikely we can immunize everyone synchronously. So then if there are always some people with low antibody levels (whose last vaccination or last infection was >6 months ago) the virus can continue to propagate through the population as a mild cold.
h/t @AndrewHires
Let's rewind the tape: '“Our data from the CDC today suggests that vaccinated people don’t carry the virus, don’t get sick and that it’s not just in clinical trials, but it’s also in real world data,” said Walensky.'
Should have consulted a biologist.
nbcbayarea.com/news/coronavir…
Should have consulted a biologist.
nbcbayarea.com/news/coronavir…
• • •
Missing some Tweet in this thread? You can try to
force a refresh