
#PFIZERLEAK - THE ISRAELI CONNECTION
(thread)
Was Dr. Robert Malone wrong about his claims about the contract between Israel and Pfizer? Does the Israeli government has an agreement not to disclose adverse events for a minimum of 10 years?
Time to set the records straight.
(thread)
Was Dr. Robert Malone wrong about his claims about the contract between Israel and Pfizer? Does the Israeli government has an agreement not to disclose adverse events for a minimum of 10 years?
Time to set the records straight.

I don't like bullies. It is one thing for someone gets upset and call you an idiot. It is completely different when a whole smear campaign is being conducted against an individual because of their believes, which is what @TheAtlantic did to @RWMaloneMD
https://twitter.com/RWMaloneMD/status/1424135220131819522
Since I was the person who was interviewed by The American Frontline Doctors which is the tweet he quoted, I thought it is time to address this disgrace of an "article". This is the hit piece of that appeared in The Atlantic, written by Tom Bartlett.
theatlantic.com/science/archiv…
theatlantic.com/science/archiv…
1) does @TheAtlantic claims @RWMaloneMD claims about Israel are misleading speculation or plainly false? Please be clear.
2) "hard to believe" is not investigative journalism, it's an opinion. Did Tom look at the facts and see what exactly is going on between Israel and Pfizer?
2) "hard to believe" is not investigative journalism, it's an opinion. Did Tom look at the facts and see what exactly is going on between Israel and Pfizer?

First, let us look at the specific case mentioned by The Atlantic.
Tom claimed that "the country’s health ministry has already warned of a link between the Pfizer shot
and rare cases of myocarditis."
What really happened? Here's the Israeli press release:
gov.il/en/Departments…
Tom claimed that "the country’s health ministry has already warned of a link between the Pfizer shot
and rare cases of myocarditis."
What really happened? Here's the Israeli press release:
gov.il/en/Departments…
Let us first look at the press release:
1) Even though myocarditis usually appears among younger men, aged 16 to 30, the report admits it started to appear among the younger age group, 16 to 19.
2) 275 cases were mentioned, 148 around the shot.
1) Even though myocarditis usually appears among younger men, aged 16 to 30, the report admits it started to appear among the younger age group, 16 to 19.
2) 275 cases were mentioned, 148 around the shot.

3) The PR mentioning the total # of individuals who got the shot is statistical fallacy. Since the majority of those who got myocarditis were from the age group of 16 to 19, there should have been focus on the # of vaccinated among that group as it is the major risk group.
4) 95% were considered to be mild cases - is it for the whole 275 cases mentioned, or for the 148?
5) Does the press release means 7 young people at the age of 16 to 19 got severe myocarditis (95% of 148) or 14 out of the total population, and if so what age where they?
5) Does the press release means 7 young people at the age of 16 to 19 got severe myocarditis (95% of 148) or 14 out of the total population, and if so what age where they?
Let's dig deeper.
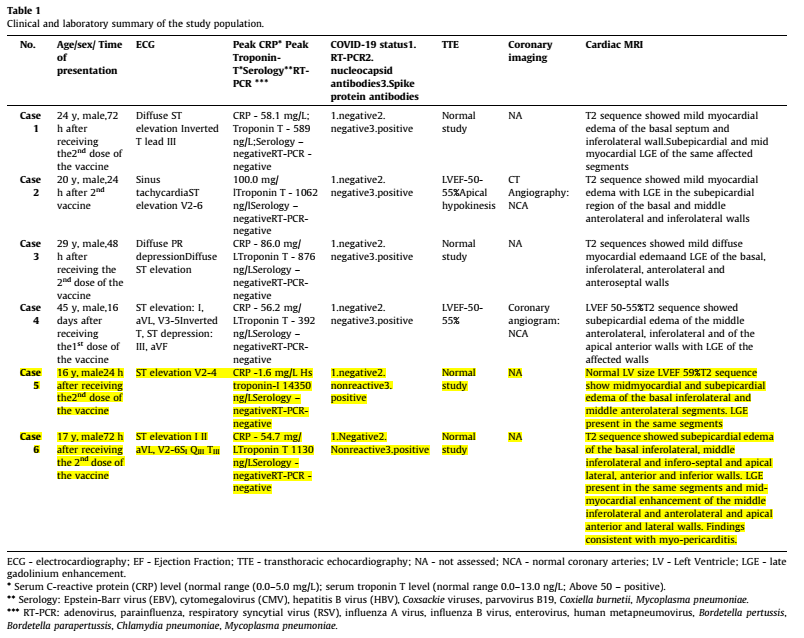
Here is the link to the epidemiological team, who published "Short Communication" called "Myocarditis following COVID-19 mRNA vaccination"
hy.health.gov.il/_Uploads/dbsAt…
Here is the link to the epidemiological team, who published "Short Communication" called "Myocarditis following COVID-19 mRNA vaccination"
hy.health.gov.il/_Uploads/dbsAt…
First, a reminder to the Ministry of health press release:
"In most cases myocarditis took the form of mild illness that passed within a few days."
"In most cases myocarditis took the form of mild illness that passed within a few days."

And here is the epidemiological team statement:
"myocarditis may have a more severe clinical presentation, may impose limitations on physical activity and may require long-term medical treatment, and follow-up"
Can you spot the difference ?????????
"myocarditis may have a more severe clinical presentation, may impose limitations on physical activity and may require long-term medical treatment, and follow-up"
Can you spot the difference ?????????

Next, the majority of the cases, as the MoH, were of young people at the age of 16 to 19, yet only two cases out of 6 which were reported about were at that group.
The selection criteria for this research is not in line with the distribution among population.
The selection criteria for this research is not in line with the distribution among population.
Next,
The hospital serve 500K, average 1.17 cases per month. 6 patients presented in less than a month.
Israel allowed 16yrs to 18yrs get the shot at the end of January.
1) How many of the 500K got the shot?
2) How many between the age 16 to 18?
3) Are the 6 the only cases?
The hospital serve 500K, average 1.17 cases per month. 6 patients presented in less than a month.
Israel allowed 16yrs to 18yrs get the shot at the end of January.
1) How many of the 500K got the shot?
2) How many between the age 16 to 18?
3) Are the 6 the only cases?

As you saw, the report of the Ministry of Health, the way it is structured and it's conclusions, alongside the very small selection group and the inability to extract meaningful information from it with regards to the real risk is weird... until you read the Pfizer contract.
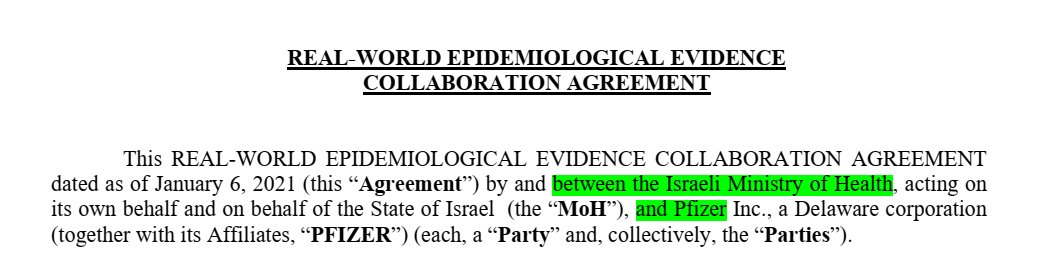
The research contract between Pfizer and Israel is called "REAL-WORLD EPIDEMIOLOGICAL EVIDENCE COLLABORATION AGREEMENT" and you can find it here:
israelhayom.co.il/sites/default/…
israelhayom.co.il/sites/default/…
The "product" are all vaccines (see #PfizerLeak for definition) for the PREVENTION of the human disease COVID-19 OR ANY OTHER DISEASE caused by SARS-CoV-2 strains, mutation, MODIFICATIONS or derivatives.
1) The product does not prevent the disease.
2) What modifications?
1) The product does not prevent the disease.
2) What modifications?

Project: epidemiological data analyses, as described
in Section 2 and Exhibit A.
Sec 2: measure and analyze epidemiological data arising from the Product.
Ex. A:
Additional subgroup analyses and vaxines effectiveness analyses, AS AGREED BY THE PARTIES.
in Section 2 and Exhibit A.
Sec 2: measure and analyze epidemiological data arising from the Product.
Ex. A:
Additional subgroup analyses and vaxines effectiveness analyses, AS AGREED BY THE PARTIES.

As you can see by the agreement above, THE PARTIES must agree to perform a test.
The Israeli MoH cannot decide to do "subgroup analysis" by itself. PFIZER NEED TO AGREE ON IT.
The Israeli MoH cannot decide to do "subgroup analysis" by itself. PFIZER NEED TO AGREE ON IT.
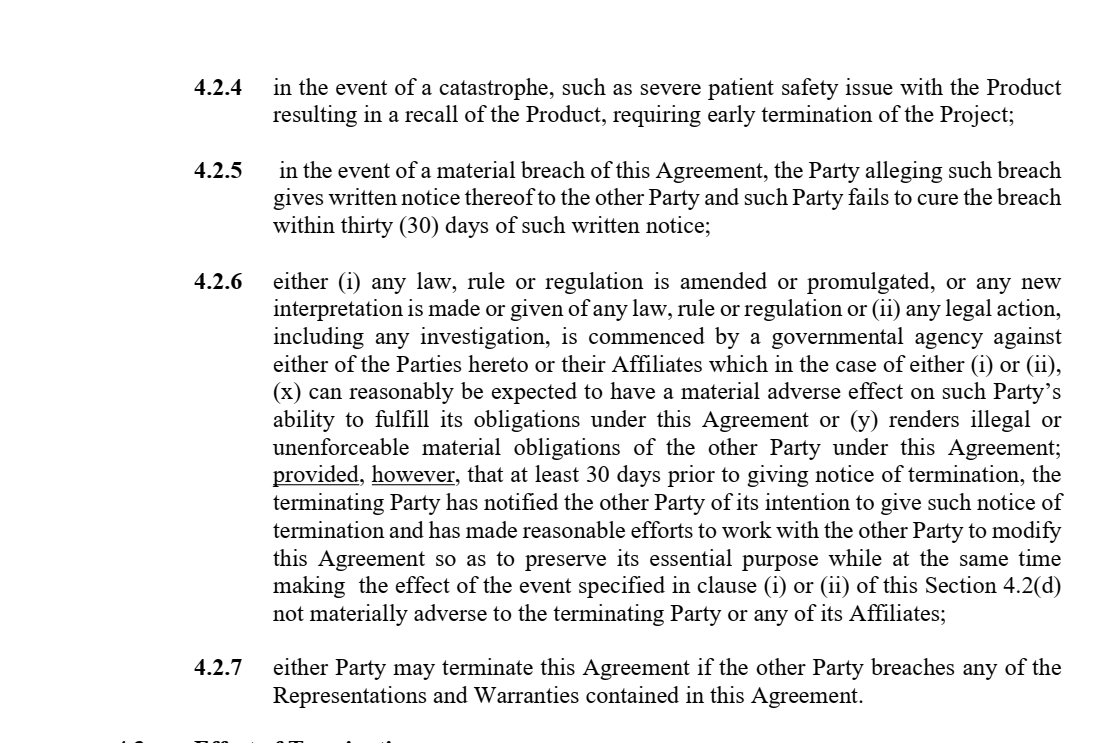
The contract seems to be indefinite, until completion of the Project (IF EVER).

Publications:
"PFIZER and MoH will jointly prepare and publish the Results in submissions) for publication, to peer-reviewed scientific or medical journals."
"PFIZER and MoH will jointly prepare and publish the Results in submissions) for publication, to peer-reviewed scientific or medical journals."

The Israeli MoH is "allowed" to communicate to the public anything OTHER THAN what they "measure and analyze (in the) epidemiological data arising from the Product rollout"
I guess the Israeli MoH can still publish the weather, right?
I guess the Israeli MoH can still publish the weather, right?



If one side want to publish epidemiological data arising from the Product rollout ON THEIR OWN (e.g. MoH), the other side must be given this in advance for it to provide comments.

Confidentiality:
Pfizer has the right to ask for "the deletion of any reference to the other Party’s Confidential Information from the proposed disclosure or publication".
Confidential: Technology, research, Pfizer Data, project data or results unless public health data.
Pfizer has the right to ask for "the deletion of any reference to the other Party’s Confidential Information from the proposed disclosure or publication".
Confidential: Technology, research, Pfizer Data, project data or results unless public health data.


"All disclosures and publications must expressly acknowledge the other Party, unless such Party objects to such acknowledgment"

THERE IS MORE BELOW!!!
Press the "Show replies"
👇👇👇
Press the "Show replies"
👇👇👇
If Pfizer & MoH does not agree on publication of information, it will need to be agreed between (someone) in Pfizer and Sharon Alroy-Preis, who works for the MoH as Israel's director of public health services.

Sharon Alroy-Preis was a co-author of "Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data"

So Sharon Alroy-Preis, the person who is suppose to negotiate in case Israel wants to publish something has been a co-author of a publication which was using the project data.
Isn't that a conflict of interest?
thelancet.com/journals/lance…
Isn't that a conflict of interest?
thelancet.com/journals/lance…
Sharon Alroy-Preis works for the MoH, who signed the manufacturing the supply agreement with Pfizer and agreed to indemnify, defend and hold harmless Pfizer...against any and all suits, claims...caused by, arising out of, relating to, or resulting from the Vaccine"
#PfizerLeak
#PfizerLeak

So, what did we learned so far?
1) @TheAtlantic "journalist" didn't do any journalism but a hit piece, without looking at the evidence.
2) Isreal's MoH reporting seems to be extremely biased towards downgrading adverse events, trying to bury them.
1) @TheAtlantic "journalist" didn't do any journalism but a hit piece, without looking at the evidence.
2) Isreal's MoH reporting seems to be extremely biased towards downgrading adverse events, trying to bury them.
3) The contract itself has no expiration date, which gives incentives to both parties to make it last as long as possible. For Israel MoH, it means people who work in the project has a job, get published in magazines (e.g. Sharon Alroy-Preis), and have no incentives to stop it.
4) There is no clear definition what is "public health data" in the contract; epidemiological data is considered to be project data, not public health data. Pfizer and MoH need to agree on new epidemiological investigations.

5) There are conflicts of interest both on MoH, who is suppose to protect Pfizer from any legal claims and yet it runs this project, and on a personal level, by assigning an individual who works for the MoH as a mediator, who also is directly involve in the project.
6) I think that what I found is much worse than the claim of the scientist who told @RWMaloneMD that the Israel and Pfizer will not disclose adverse events for a minimum of 10 years. The research contract is heavily redacted & the Manufacturing & supply contract was not exposed.
7) I INVITE YOU TO READ THE EVIDENCE AND DECIDE FOR YOURSELF.
Finally, @RWMaloneMD - thank you for your courage for speaking out and withstanding the waves of slur. What an inspiration.
THE TRUTH SHALL SET YOU FREE.
Ehden Biber,
Also @ T.ME/EH_DEN
Finally, @RWMaloneMD - thank you for your courage for speaking out and withstanding the waves of slur. What an inspiration.
THE TRUTH SHALL SET YOU FREE.
Ehden Biber,
Also @ T.ME/EH_DEN
As was brought to my attention, this smear job was supported by grants from Chan Zuckerberg Initiative and the Robert Johnson Foundation, a member of the World Economic Forum (WEF).
"It's a big club, and you ain't in it!" (George Carlin).
"It's a big club, and you ain't in it!" (George Carlin).

#PFIZERLEAK - THE ISRAELI CONNECTION - APPENDIX A.
BLOG POST ABOUT THE BRAZILIAN CONTRACT:
✓ STEP-BY-STEP VALIDATION OF THE CONTRACT
✓ ANALYSIS OF CONTRACT CLAUSES
✓ STATEMENT BY SENIOR PFIZER EXECUTIVE ALL COUNTRIES SIGNED SUCH CONTRACT
#PfizerLeak
BLOG POST ABOUT THE BRAZILIAN CONTRACT:
✓ STEP-BY-STEP VALIDATION OF THE CONTRACT
✓ ANALYSIS OF CONTRACT CLAUSES
✓ STATEMENT BY SENIOR PFIZER EXECUTIVE ALL COUNTRIES SIGNED SUCH CONTRACT
#PfizerLeak
https://twitter.com/eh_den/status/1428832501091508226?s=19
#PFIZERLEAK - THE ISRAELI CONNECTION - APPENDIX B.
PFIZERLEAK REDUX - YOUR DEMOCRACY IS IN DANGER!
THE REAL REASON WHY YOUR GOVERNMENT KEEPS THE PFIZER MANUFACTURING AND SUPPLY CONTRACTS SECRET FOR 10 YEARS.
PFIZERLEAK REDUX - YOUR DEMOCRACY IS IN DANGER!
THE REAL REASON WHY YOUR GOVERNMENT KEEPS THE PFIZER MANUFACTURING AND SUPPLY CONTRACTS SECRET FOR 10 YEARS.
https://twitter.com/eh_den/status/1426254971876610055?s=19
#PFIZERLEAK - THE ISRAELI CONNECTION - APPENDIX C.
COPTIGATE - THE WORST DESIGN FLAW IN HUMAN HISTORY THAT IS IMPACTING YOUR HEALTH.
How come manufacturers are using a technology that both they and the regulators know will cause unknown, risky results?
COPTIGATE - THE WORST DESIGN FLAW IN HUMAN HISTORY THAT IS IMPACTING YOUR HEALTH.
How come manufacturers are using a technology that both they and the regulators know will cause unknown, risky results?
https://twitter.com/eh_den/status/1426885632140394499
• • •
Missing some Tweet in this thread? You can try to
force a refresh

















