There is a lot of concern/confusion about vaccine effectiveness against the delta variant. How effective are the vaccines against Delta & how to interpret real-world observational data? So much misinformation is being circulated, so this thread brings key data together. 🧵(1/n)
Vaccine efficacy measures the relative reduction in infection/disease for the vaccinated vs unvaccinated arm. For instance, a vaccine that eliminates all risk would have an efficacy of 100%. Efficacy of 50% means you have a 50% reduced risk compared to an unvaxxed person. (2/n) 

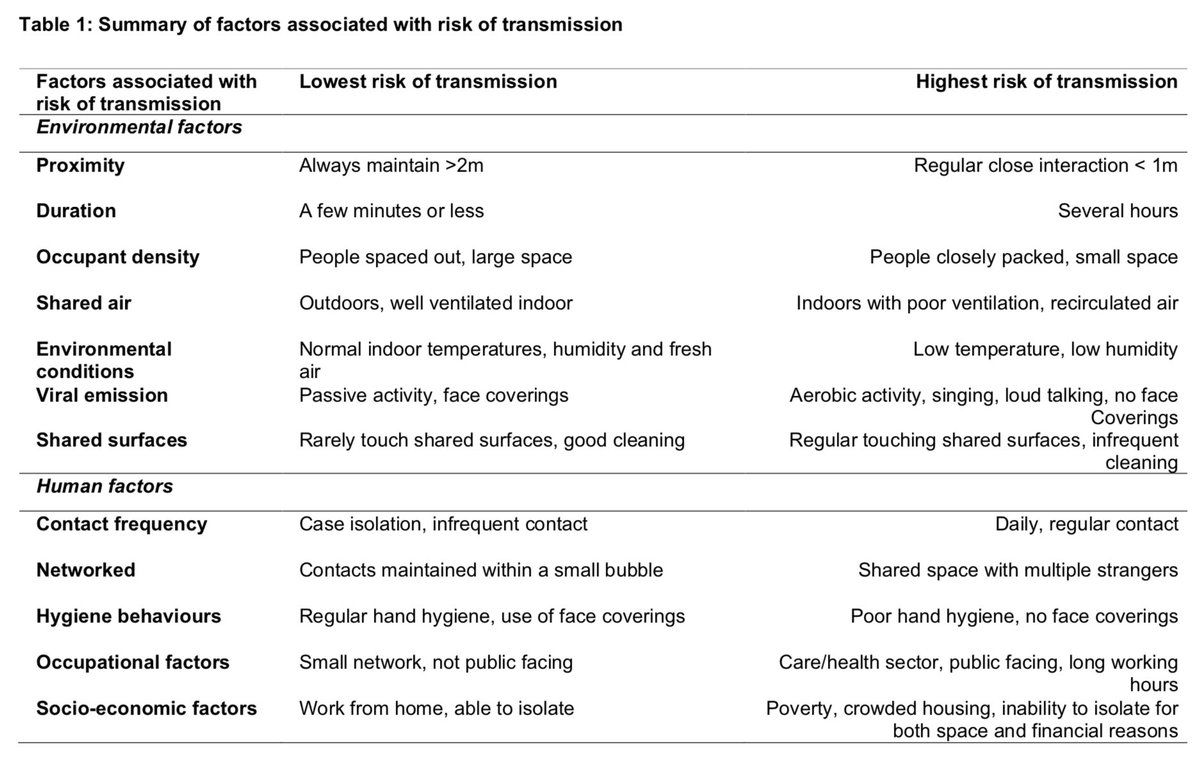
All studies assessing the performance of vaccines against Delta are based on real-world data (vaccine effectiveness), which are influenced by variant transmissibility, human behaviour, and immunity status of the population, therefore they require careful interpretation. (3/n)

Vaccines are designed to protect symptomatic illness; therefore, the vaccine effectiveness (VE) is often referred to as the performance against this primary endpoint. But some studies also report VE against hospitalisation and infection, which I will report separately. (4/n)
1- Vaccine effectiveness (VE) against hospitalisation:
The evidence so far suggests that VE against hospitalisations is highly preserved against Delta. As you can see in this figure, high protection against hospitalisation (>80%) is maintained after the 2nd dose. (5/n)
The evidence so far suggests that VE against hospitalisations is highly preserved against Delta. As you can see in this figure, high protection against hospitalisation (>80%) is maintained after the 2nd dose. (5/n)

2- VE against symptomatic illness:
This is also very similar across the board, demonstrating preserved effectiveness against symptomatic Delta w/the Israel data being an outlier, for which we have yet to see methods/details. Let’s take a look at these studies. (6/n)
This is also very similar across the board, demonstrating preserved effectiveness against symptomatic Delta w/the Israel data being an outlier, for which we have yet to see methods/details. Let’s take a look at these studies. (6/n)

A test-negative case-control analysis from England demonstrate that after the 2nd dose of Pfizer and Oxford vaccines, effectiveness against symptomatic delta illness remained high, with a modest decline observed w/ delta compared to alpha. (7/n)
nejm.org/doi/full/10.10…
nejm.org/doi/full/10.10…

A study from Canada also showed preserved VE against symptomatic delta illness w/ a modest decline compared to alpha. Both studies showed reduced protection against symptomatic illness w/ 1st dose, but VE recovered after the 2nd dose. (8/n)
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…

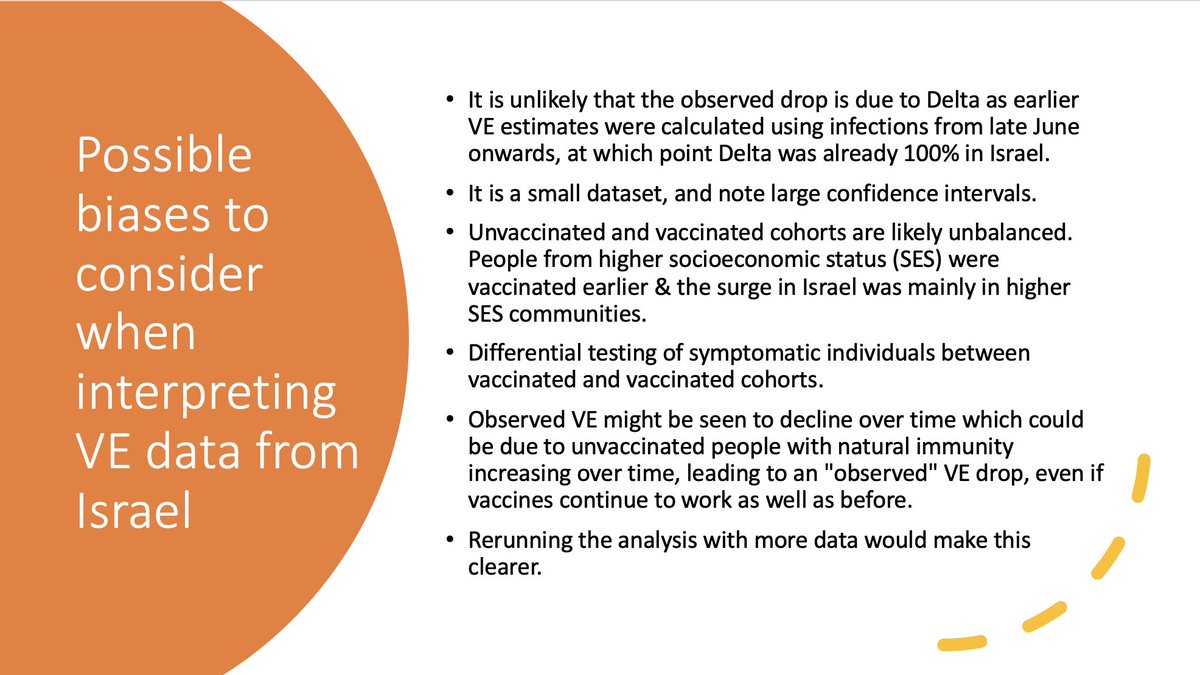
Data published by the Israel MoH caused a lot of concern, suggesting that the Pfizer VE against symptomatic infection fell to 40%, lower than seen in other studies. While we have yet to see details of this analysis, there are likely several confounders to consider. (9/n)
3- VE against infection:
This measures all PCR +ve cases that are observed in vaccinated vs unvaccinated group, regardless of symptoms. These cases also include those who briefly become swab +ve before the immune system kicks in, but never develop any symptoms or illness. (10/n)
This measures all PCR +ve cases that are observed in vaccinated vs unvaccinated group, regardless of symptoms. These cases also include those who briefly become swab +ve before the immune system kicks in, but never develop any symptoms or illness. (10/n)
Unfortunately, there has been very little systematic evaluation of VE against asymptomatic swab positivity. These estimates are affected by various biases such as testing criteria, behaviour, exposure risk, immunity status, and community prevalence. (11/n)
So, it needs to be recognised that VE for infection is a dynamic figure influenced by several factors, thus estimates vary quite a lot. Pre-delta studies showed estimated 55-80% VE against infection, and there is a modest decline seen w/delta. (12/n)
academic.oup.com/ofid/advance-a…
academic.oup.com/ofid/advance-a…

Recent UK analysis based on systematic testing demonstrate that Pfizer & Oxford vaccines remain highly protective against any PCR +ve infection, similar VE seen w/Alpha vs Delta, including those with Ct <30 (high viral load). (13/n)
ndm.ox.ac.uk/files/coronavi…
ndm.ox.ac.uk/files/coronavi…

According to REACT data (a random sample of the population in England), VE against swab positivity was 58% (for strong positives). In this study, 1 in 25 double-vaxxed individuals (3.8%) tested swab-positive after covid exposure. (14/n)
spiral.imperial.ac.uk/handle/10044/1…
spiral.imperial.ac.uk/handle/10044/1…

A test-negative case-control study from Qatar demonstrated high effectiveness against swab positivity with delta, 60% w/ Pfizer and 86% w/ Moderna. However, follow up period may not be the same for both vax groups. (15/n)
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…

According to Mayo clinic data, based on routine patient-initiated testing, 2 doses of mRNA vaccines still provide high effectiveness against infection, 76% w/Moderna and 42% w/Pfizer vaccines. Follow up period may not be the same for both vax groups (16/n)
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…

In a nursing home resident cohort in the US (routine surveillance data), 2 doses of mRNA vaccines were 75% effective against infection in early 2021, which declined to 53% when Delta predominated. (17/n)
cdc.gov/mmwr/volumes/7…
cdc.gov/mmwr/volumes/7…

Based on routine surveillance data in NYC, the overall age-adjusted vaccine effectiveness against infection was 80% w/delta and some waning was seen in recent months in 18-49yo. However, these analyses didn't account for prior infection in unvaxxed (18/n)
cdc.gov/mmwr/volumes/7…
cdc.gov/mmwr/volumes/7…

Finally, recent data based on breakthrough infections in Utah showed an estimated 82% VE against infection, w/ a modest reduction corresponding to delta expansion. (19/n) medrxiv.org/content/10.110…

In summary, currently available vaccines work exceptionally well against Delta w/ high effectiveness demonstrated for symptomatic illness and hospitalisation. They also show high effectiveness in preventing swab positivity w/a modest decline likely due to Delta. (20/n)
While the modest decline in effectiveness against infection causes some concern, as discussed, VE for infection is a dynamic figure & changes over time. Therefore, it is inaccurate to reference a single percentage & imply a massive reduction against infection due to delta. (21/n)
There are also concerns about waning immunity; however, this often refers to effectiveness against infection, not symptomatic or severe illness. And it’s critical to consider caveats when interpreting these results. (22/n)
https://twitter.com/jburnmurdoch/status/1429878189011111936?s=20
What we’re observing is very much aligned w/prior knowledge. Protection from symptomatic illness is easier to achieve than infection. B/c while neutralising Abs decrease over time, protective immunity provided by memory T/B cells is preserved & expected to be long-lasting (23/n)

It is essential to remember vaccines do not work to bounce incoming virus particles off you. And even if infected, vaccines continue to provide significant protection against symptomatic illness and hospitalisations. END
https://twitter.com/Ryan_Mac_Phd/status/1425798129673179141?s=20
Addendum: According to a new pre-print, Israel data now pretty much align w/ data from UK/US. VE for severe disease is still >85% after 6m, VE for infection wanes over time. VE for symptomatic illness is not interpretable as discussed in tweet #9. (25/n)
https://twitter.com/_lewisy/status/1430291436172455939?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh